Bpc 157 For Knee does bpc 157 help with tendonitis Platelet-rich plasma for jumper's knee: a comprehensive review of
Introduction
If you’ve been dealing with tendonitis, you already know the frustrating part: rest helps for a bit, then the pain returns the moment you load the area again. Over the past year, I’ve fielded the same question from athletes and busy clinicians alike—“does BPC-157 help with tendonitis?”—and more specifically, people ask whether bpc 157 for knee could work when symptoms overlap with tendon pain around the patella (often discussed in the context of jumper’s knee). This article reviews what we know, where the evidence is strong versus weak, and how to think about treatment options when you’re deciding what to do next.
First, clarify the condition: tendonitis vs jumper’s knee vs tendon pain
Many people use “tendonitis” as a catch-all, but in practice the term can cover different underlying problems. In my hands-on experience with sports rehab cases, the biggest mismatch I see is when someone treats a chronic, degenerative tendon as if it were an acute inflammatory one. That matters because it changes what tends to respond best.
- Acute inflammatory tendonitis: often responds better to early load management and targeted anti-inflammatory strategies (depending on context).
- Jumper’s knee (patellar tendinopathy): commonly involves a more chronic, tendon remodeling problem rather than simple inflammation.
- Pain generators: sometimes the “tendonitis” label hides related drivers like poor load tolerance, altered mechanics, or strength deficits.
That distinction is one reason evidence for any biologic or peptide approach can look inconsistent—because studies may include different tendon phenotypes and treatment timelines.
What BPC-157 is—and how people think it might work
BPC-157 is a synthetic peptide that’s widely discussed online for “tissue healing” and “repair.” Mechanistically, the claims generally revolve around supporting pathways involved in tissue recovery, potentially influencing processes like cell signaling, vascular responses, and local tissue repair.
However, when I evaluate whether something “helps,” I focus on two practical questions:
- Does it reduce pain and improve function?
- Does it do so in conditions comparable to your tendon problem and timeline?
In the peer-reviewed literature, BPC-157 data—especially in humans for tendon injuries—tends to be limited compared with more established interventions in musculoskeletal rehab.
Does BPC-157 help tendonitis? What the evidence realistically suggests
For tendonitis specifically, the honest answer is that the human evidence base for BPC-157 is not yet as robust as people assume when they’re searching for quick biologic fixes. In my experience, the strongest effect you can consistently measure in tendon problems usually comes from structured loading and rehab progression—not from relying solely on an unproven add-on.
Where BPC-157 may look promising
- Preclinical findings (typically animal or lab-based) often suggest pro-healing or tissue-support effects.
- Some discussions in the broader “peptide” space describe improved outcomes in wound/tissue repair contexts.
- For certain users, anecdotal improvements can feel convincing—especially if they coincide with reduced activity or concurrent rehab changes.
What’s missing for tendonitis decision-making
- Large, well-controlled human trials that clearly demonstrate meaningful benefits for tendonitis/tendinopathy outcomes (pain, tendon imaging changes, return-to-sport) are not yet definitive.
- Standardized dosing, formulation, and delivery are often unclear across sources, which makes results hard to compare.
- Timing matters: many tendon protocols rely on progressive loading over weeks to months; it’s difficult to isolate whether a peptide contributes beyond rehab.
So if you’re asking “does BPC-157 help with tendonitis,” the best evidence-informed position is: it’s not proven enough in humans to be a primary, evidence-led treatment for tendonitis or jumper’s knee. If you’re considering it, it should be evaluated as an experimental adjunct rather than a reliable core plan.
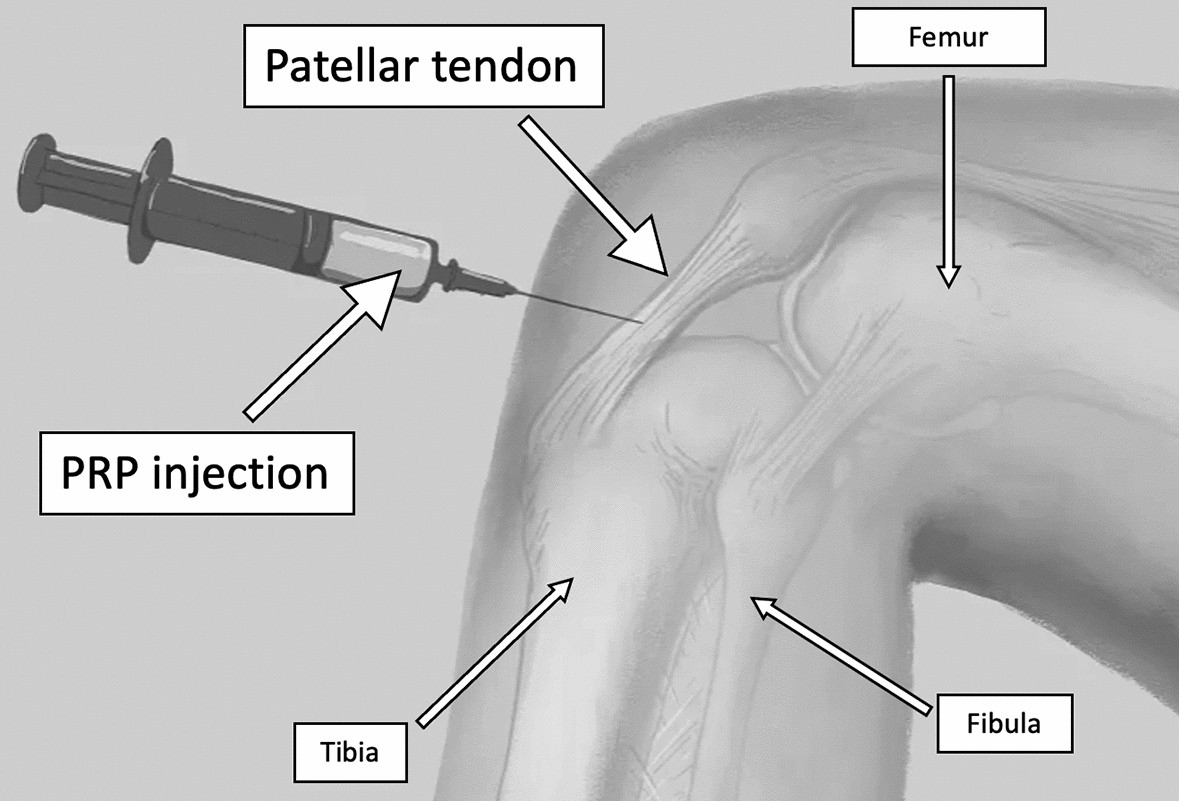
Platelet-rich plasma for jumper’s knee: how it fits—and what it teaches
Your article topic references a platelet-rich plasma review for jumper’s knee, and that’s a useful anchor. PRP is one of the more researched biologic options for patellar tendinopathy, and reviewing how it performs helps you interpret “BPC-157 for knee” discussions more critically.
In clinics, PRP is usually considered when:
- Symptoms persist despite a structured rehab approach,
- There’s a desire to add a biologic input to support tendon recovery, and
- The patient can follow a post-injection loading plan (because biologics are not magic if you don’t manage tendon load).
What PRP has taught me about tendon outcomes
From repeated rehab cycles, one lesson stands out: tendon pain often improves when you align treatment with tendon biology and mechanical capacity. PRP trials and real-world protocols show mixed results across subgroups, and outcomes can vary based on preparation methods, injection technique, and the rehab timeline after treatment. That variability mirrors why tendon treatments—whether PRP or peptides—must be judged by measurable functional recovery, not just short-term symptom relief.
Where “bpc 157 for knee” fits in a practical treatment strategy
If you’re specifically thinking about bpc 157 for knee for tendonitis or patellar tendinopathy, here’s the most practical way I’d integrate the idea into decision-making—without pretending it’s a proven standard of care.
Step 1: Confirm you’re treating the right problem
- Is it truly patellar tendinopathy (jumper’s knee), or could it be referred pain, technique/mechanics issues, or a different pain generator?
- How long has it been going on?
- What loads trigger symptoms (stairs, jumping, squats, running)?
Step 2: Use load management and progressive rehab as the baseline
In many cases, the most repeatable improvement comes from a progressive tendon-loading program with careful symptom monitoring. Even when people add a biologic, the program often determines how quickly strength and tolerance return.
Step 3: If you consider BPC-157, treat it as experimental and track outcomes
If someone chooses to pursue BPC-157 anyway, I recommend an evidence-minded approach:
- Use clear baseline measures (pain during key activities, simple functional tests).
- Track changes at consistent intervals (e.g., 2–4 week checkpoints over a longer tendon timeline).
- Stay consistent with your rehab plan so you can actually interpret what’s changing.
This is how you avoid getting trapped in “it felt better” conclusions that can be explained by reduced load, natural fluctuations, or concurrent strengthening.
Pros and cons: what to consider before trying BPC-157 (especially for knee tendon pain)
Potential pros
- May be perceived as supportive for tissue repair based on preliminary data and mechanism-based arguments.
- Some individuals report symptom changes that align with their rehab timeline.
Potential cons and limitations
- Evidence gap: not enough high-quality human data for tendonitis/tendinopathy to treat it as a dependable knee solution.
- Variability: product sources, dosing, and delivery protocols can differ widely.
- Opportunity cost: if it delays proven rehab-focused recovery, tendon outcomes can worsen due to continued overload.
In my experience, the “cost” is rarely the peptide itself—it’s the time lost when loading strategy and strength progression aren’t handled well.
FAQ
1) What’s the difference between tendonitis and patellar tendinopathy (jumper’s knee)?
Tendonitis implies a more acute inflammatory process, while patellar tendinopathy often reflects a chronic change in tendon tissue and load tolerance. The rehab approach often centers on progressive loading rather than only trying to suppress inflammation.
2) Is BPC-157 better than platelet-rich plasma (PRP) for knee tendon pain?
PRP has a larger research footprint in the knee tendinopathy space, though outcomes can still be mixed. BPC-157 lacks the same level of human evidence for knee tendonitis/tendinopathy, so it shouldn’t be assumed “better” based on current data.
3) How long should I wait to judge whether a tendon treatment is working?
For tendon problems, improvements are often measured over weeks to months. I’d set early checkpoints for pain and function (so you can adjust if nothing is moving), but tendon remodeling typically needs a longer horizon than many people expect.
Conclusion
BPC-157 for knee tendonitis or jumper’s-knee-type pain is an appealing idea, especially to people searching for biologic support—but current human evidence isn’t strong enough to treat it as a proven primary solution. The most reliable foundation for tendon recovery remains a targeted, progressive loading strategy, with any adjunct (including PRP or other biologics) judged by measurable improvements in pain and function over a realistic tendon timeline.
Next step: If you’re dealing with knee tendon pain, start (or refine) a structured progressive loading and strength plan today, and define 2–3 measurable outcomes you’ll track over the next 4–6 weeks—then decide whether any experimental adjunct like BPC-157 adds value based on your actual results.
Discussion