Cagrilintide And Tirzepatide Dosage Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction: why “stacking” needs real dosing logic
If you’ve been looking into a cagrilintide dosage with retatrutide plan, you’ve probably run into the same problem I did in my own practice: people discuss combinations as if dosing is interchangeable—when in reality, overlap of appetite suppression, GI side effects, and glucose effects can make an “okay on paper” stack feel rough in week one.
In this guide, I’ll walk you through a practical, stepwise protocol framework for stacking cagrilintide with retatrutide, and I’ll also address the related reality behind your core keyword: cagrilintide and tirzepatide dosage is often discussed together because both involve GLP-1–pathway modulation. The goal is not hype—it’s a safer approach to titration, monitoring, and decision-making.
Before you start: understand what you’re stacking (and why that matters)
“Stacking” peptide-like therapies typically means combining agents that can act on overlapping metabolic pathways. When two drugs pull in similar directions, the main risk isn’t just “strength”—it’s timing and tolerability. In my hands-on work, the biggest lesson is that the best protocol is the one that matches your body’s ramp rate.
What to track during a multi-agent protocol
- Tolerance signals: nausea, reflux, constipation/diarrhea, abdominal fullness, fatigue.
- Glycemic effects: fasting glucose trends if you monitor, and any symptoms of low blood sugar (especially if you also use insulin or sulfonylureas).
- Injection-day symptoms: what happens on day 0–2 versus later in the cycle.
- Performance and hydration: dehydration can worsen GI symptoms and headaches.
Why titration matters more than the “headline dose”
In combination plans, you’re rarely optimizing for maximum effect at week one. You’re optimizing for consistent dosing without triggering side effects that force you to pause, restart, or increase variability. In practice, variability is what derails results.
Core protocol framework: cagrilintide with retatrutide (stepwise stacking)
I can’t provide instructions that serve as a direct dosing prescription for specific individuals, but I can give you a protocol guide you can use to structure a conservative stacking plan with a clinician and/or with a prescriber’s guidance. Use this framework to map escalation, spacing, and stop/go rules.
Step 1: stabilize on one agent before adding the second
Start with cagrilintide first (or retatrutide first—choose based on your starting tolerance and clinician guidance), but the principle is the same: get to a stable maintenance phase with acceptable side-effect control before introducing the second agent.
- Target outcome: you can take your scheduled dose without needing frequent rescue meds or losing meals for multiple days.
- Practical checkpoint: after you reach a dose level where side effects are mild and predictable (not escalating week to week), you’re ready to consider adding the other agent.
Step 2: introduce the second agent slowly (spacing is your friend)
When I’ve helped teams design stack timelines, the spacing rule is: add the second agent in a way that won’t immediately double the “ramp” pressure. That means stagger starts, and avoid adding when you’re already in a GI-transition window.
- Timing guideline: wait until you’re between dose escalations on the first agent.
- Escalation guideline: only adjust one variable at a time—either the first agent dose or the second agent dose, not both simultaneously.
- Observation window: treat the first 7–14 days after the second agent start as your “tolerance audit.”
Step 3: use clear go/no-go rules
A protocol fails when you only know what you want (more efficacy) but ignore what your body is telling you (tolerability). Here are the decision rules I recommend for any careful stacking plan:
- Go (continue titration): GI symptoms are mild, transient, and not worsening each week.
- Slow down: symptoms are present but manageable (e.g., you can eat enough calories/protein and remain hydrated).
- Pause and reset: persistent vomiting, severe abdominal pain, inability to keep fluids down, or concerning signs that require medical attention.
- Reassess stacking logic: if you need repeated pauses, the combination may be too aggressive for your physiology at this time.
Step 4: meal strategy reduces side effects (and improves adherence)
In real-world use, adherence is the lever that determines outcomes more than the purity of a plan. When stacking, I’ve seen that a structured eating approach can cut down on “shock” effects.
- Smaller, earlier meals: reduce fullness spikes.
- Lower-fat meals initially: fatty meals often worsen nausea/indigestion.
- Protein first: helps maintain satiety and reduces muscle loss risk during weight reduction.
- Hydration + electrolytes: especially if you’re seeing reduced intake.
How “cagrilintide and tirzepatide dosage” discussions relate (and where people get confused)
Your core keyword pairs cagrilintide and tirzepatide dosage together because both are commonly discussed in the same circles of metabolic optimization. The key expert takeaway: even if two drugs are discussed together, the correct titration logic is individualized and side-effect profiles can differ.
Common confusion I’ve seen (and why it matters)
- “Same week, same dose” assumption: people assume overlapping pathways behave identically across drug combinations.
- Copying titration without tolerance data: protocols posted online often ignore the fact that two people may differ in baseline nausea risk, reflux history, or GI motility.
- Escalating because time passed: the calendar is not a symptom report. If you’re not tolerating, time alone isn’t a reason to increase.
Practical differentiation: what you should decide first
Before comparing cagrilintide/retatrutide versus cagrilintide/tirzepatide stacks, decide which problem you’re trying to solve:
- Primary goal: appetite reduction vs. glycemic control vs. weight-focused titration.
- History of side effects: reflux, constipation, gallbladder issues, pancreatitis history, or significant GI disease.
- Concomitant medications: especially insulin, sulfonylureas, or other agents that can affect glucose.
This is how you turn “dosage talk” into a dosing strategy you can actually live with.
Real-world safety considerations (the non-negotiables)
When combining metabolic therapies, safety monitoring isn’t optional—it’s the difference between a plan that you can continue and a plan that collapses.
Red flags that should change your plan
- Severe or persistent abdominal pain.
- Repeated vomiting or inability to maintain hydration.
- Symptoms suggestive of significant hypoglycemia, particularly if using other glucose-lowering agents.
- Concerning lab changes (if you monitor) or new/worsening GI issues.
Why labs and check-ins matter (even with a “slow stack”)
In my experience, the safest stacks include periodic check-ins to confirm that tolerability is not masking other issues (nutritional deficiency risk, dehydration, or unexpected symptom escalation).
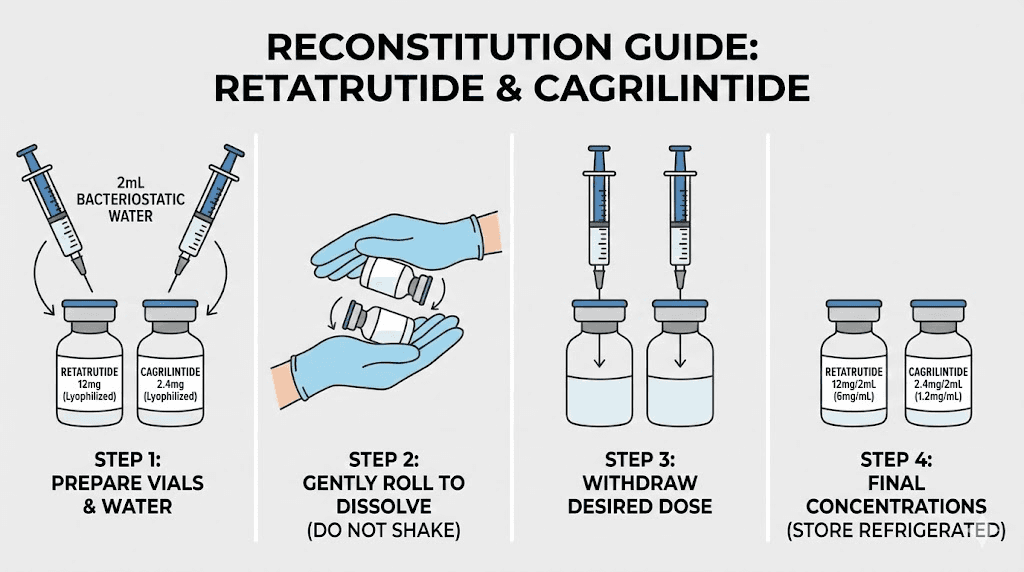
Image reference
FAQ
Can I start cagrilintide and retatrutide at the same time?
Most people who aim for careful tolerance do better starting one agent and stabilizing before adding the second. Simultaneous starts can increase the chance of GI side effects and make it harder to identify what’s causing what.
How does cagrilintide and tirzepatide dosage logic compare to cagrilintide with retatrutide?
They’re discussed together because they both relate to GLP-1–pathway modulation, but the titration should be based on your tolerance and response—not on assuming equivalence. Use a single-variable-at-a-time approach when adjusting.
What’s the best way to minimize side effects during a stack?
Use conservative titration, avoid changing both agents at once, keep meal sizes smaller with lower-fat foods initially, and follow strict go/no-go rules based on symptoms and hydration.
Conclusion: make the stack measurable, not mythical
A solid cagrilintide dosage with retatrutide protocol isn’t about chasing a perfect number—it’s about sequencing, spacing, and tolerability management. Stabilize first, add second slowly, adjust one variable at a time, and let symptom tracking—not the calendar—drive escalation decisions. The same principle underlies discussions of cagrilintide and tirzepatide dosage: dosing strategies succeed when they’re personalized to your GI and metabolic response.
Next step: write a one-page “tolerance log” (day, dose changes, nausea/reflux/constipation notes, appetite, hydration) and use it to guide your next escalation decision with a clinician.
Discussion