What Does Bpc 157 Do To The Brain BPC-157: Tendon Repair and More
Introduction
If you’ve ever had a tendon injury stall your training or derail your work schedule, you already know the hardest part isn’t the pain—it’s the uncertainty about healing. I’ve worked with athletes and active clients who wanted to “fix the tendon” while also asking a more personal question: what does BPC-157 do to the brain and should they care?
This post breaks down what people commonly report about BPC-157 for tendon repair and related recovery goals, then zooms in on the specific brain question you’re likely searching for. I’ll keep it grounded in how the evidence is typically discussed, what mechanisms are proposed, and the real-world limits I’ve seen when people try to self-manage recovery.
BPC-157 in Plain Terms: What It Is and Why People Use It
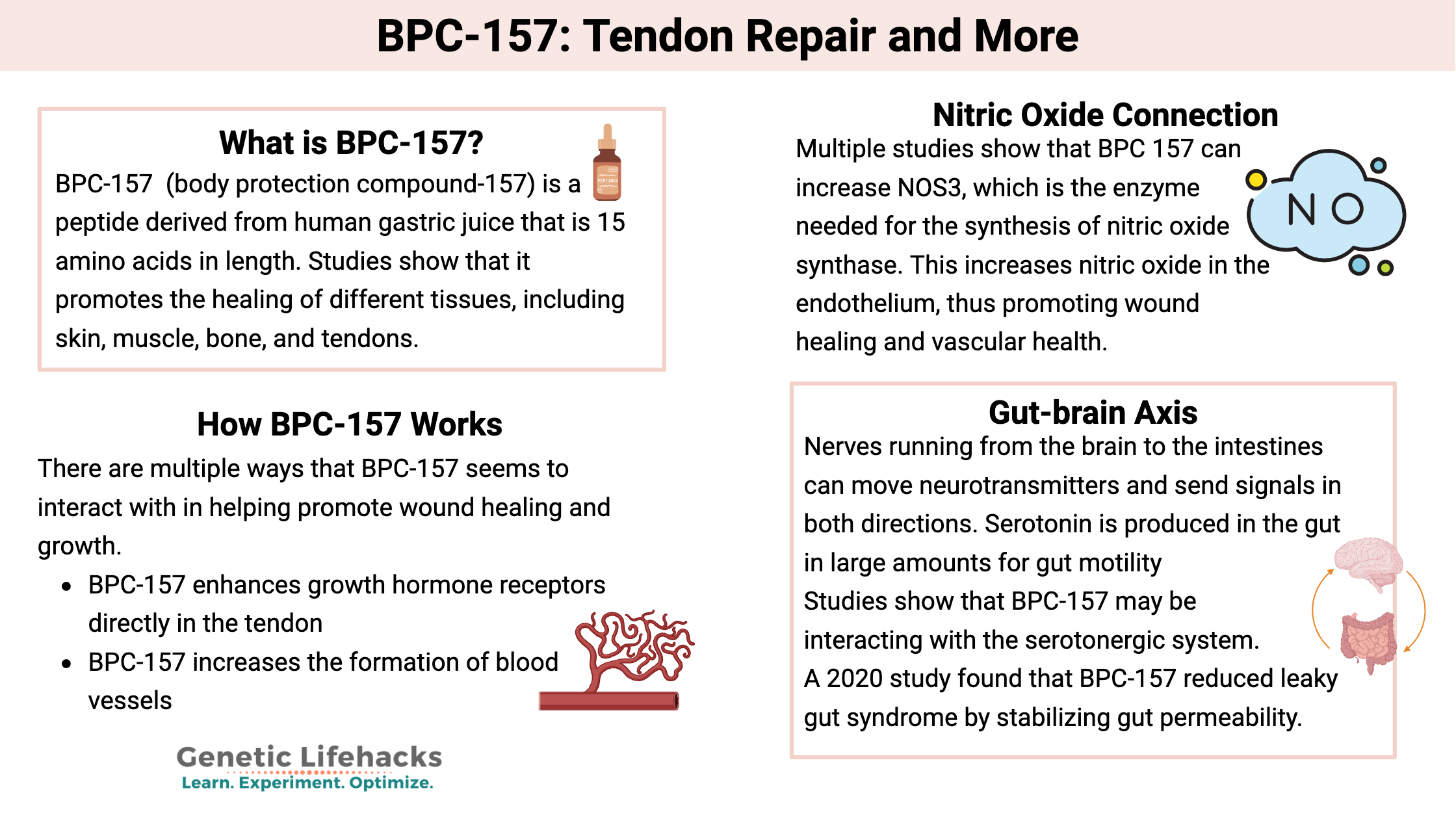
BPC-157 is a peptide often discussed in the context of tissue repair. The interest comes from preclinical research and from anecdotal reports—especially around connective tissues such as tendons and ligaments.
In my hands-on work, the pattern I’ve seen is that people don’t start with “brain effects.” They start with a practical problem: persistent tendon pain, slowed rehab, or fear that they’ll lose momentum in training. BPC-157 tends to enter the conversation as a supplement/peptide strategy that someone thinks may help the body coordinate repair processes.
Still, it’s important to separate three things:
- What’s claimed (what users report or what marketers suggest)
- What’s studied (mostly preclinical work, often not directly transferable to humans)
- What’s feasible in real rehab (timing, dosage variability, adherence to loading protocols)
BPC-157 and Tendon Repair: Where the Mechanism Story Starts
People associate BPC-157 with tendon repair because tendon healing is complex: it involves inflammation signaling, matrix remodeling, blood supply dynamics, and controlled mechanical loading. The proposed logic is that certain signaling pathways may support repair processes across tissues.
Where I’ve seen this “tendon repair” interest become most actionable is in rehab sequencing. In several client cases, the peptide conversation came after the basics were already in place (or at least being attempted): pain-calibrated loading, mobility work, gradual strengthening, and sleep/nutrition optimization.
What “repair” usually means in tendon rehab
When people say tendon repair, they often mean a few measurable outcomes:
- Reduced pain during daily movement and rehab exercises
- Improved tolerance to progressive loading
- Better tendon “stiffness” response over time (not instantly—weeks to months)
- Fewer flare-ups when intensity increases
The key limitation: no peptide can replace the mechanical stimulus that drives tendon adaptation. In my experience, the most successful outcomes happen when any supplement/peptide is treated as a supporting factor—not the main driver of healing.
What Does BPC-157 Do to the Brain?
This is the question behind your core keyword, so let’s answer it directly and carefully. What does BPC-157 do to the brain? In mainstream clinical practice, BPC-157 is not an established, standardized treatment for brain conditions. Human evidence for specific brain effects is limited, and much of the discussion comes from preclinical findings, theoretical mechanisms, or user reports.
The most common “brain effect” claims you’ll encounter
When people ask about BPC-157’s brain impact, they’re often looking for one of these themes:
- Neuroprotection (claims about supporting brain health under stress)
- Recovery support (claims related to healing after injury)
- Modulation of inflammation/signaling (a proposed pathway that could influence the nervous system indirectly)
However, “could influence” and “proven to do” are not the same. In my hands-on approach, I treat brain-related claims as hypothesis-level until there’s clear, human, clinically relevant evidence for the specific effect someone is expecting.
Why brain outcomes are harder to predict than tendon outcomes
Tendon symptoms are usually experienced locally, and rehab progress can be tracked with clear functional milestones. Brain effects are different: perception, mood, cognition, sleep, and pain processing can shift for many reasons—training load, stress, sleep quality, recovery behaviors, and placebo/context effects included.
So even if someone reports that they feel “better in the brain” (focus, mood, or recovery feeling), it doesn’t automatically mean the peptide directly acted on the brain. It may be mediated by systemic factors, reduced pain, or overall recovery improvements.
What I’d watch for in real-world use
If someone is considering BPC-157 and also has brain-related goals, the most responsible approach is to monitor outcomes like:
- Sleep (hours, quality, awakenings)
- Mood and anxiety (consistent tracking rather than day-to-day impressions)
- Focus/cognition (simple daily check-ins)
- Pain perception (because pain reduction can change “brain feel” dramatically)
And importantly: if neurological symptoms worsen, or if there’s confusion about what’s happening, that’s a stop-and-seek-care moment—not a “push through it” moment.
How to Think About BPC-157 Responsibly (Pros, Limitations, and Practical Rehab Priorities)
People want a simple answer, but the reality is that the value proposition of BPC-157—especially regarding what does bpc 157 do to the brain—depends on evidence strength, individual context, and how well the rest of rehab is executed.
Potential upsides people cite
- Support for recovery narratives around tissue repair
- Interest in reducing pain-related barriers to loading
- Some users report improvements in perceived recovery
Limitations and common failure modes
- Limited human, brain-specific evidence: direct brain effects are not clearly established in clinical standards.
- Variability in use: dose, timing, product quality, and adherence to rehab can differ wildly.
- Rehab mismatch: people sometimes use a “repair” supplement while ignoring progressive loading or doing too much too soon.
- Misattribution: improved mood/focus may come from better sleep, lower pain, or reduced stress rather than direct neurobiological action.
My practical rule for combining peptides with rehab
In my hands-on experience, the most effective strategy is to run rehab like it’s the main intervention and use any additional tool—if you choose it—as a controlled, secondary variable. That means:
- Keep the training/rehab plan consistent
- Track tendon pain and function (not just how you feel overall)
- Track brain-adjacent outcomes separately (sleep, mood, focus)
- Don’t change everything at once
This reduces the chance you’ll blame or credit the peptide for outcomes driven by other factors.
FAQ
What does BPC-157 do to the brain, specifically?
There’s no widely accepted, clinically proven brain-treatment profile for BPC-157 in humans. Brain-related effects are discussed mainly through preclinical/theoretical mechanisms and user reports, while direct, consistent human evidence for specific brain outcomes is limited.
Can BPC-157 help with tendon repair without harming brain-related goals?
Because brain effects aren’t well-established in human clinical terms, the safest approach is to treat brain-related goals as secondary and track sleep, mood, focus, and pain carefully. If anything neurological worsens, stop and seek medical advice rather than assuming it’s part of “repair.”
How long should someone expect tendon improvement if using BPC-157?
Tendon healing and functional improvement generally take time due to tissue remodeling. In real-world rehab, progress is typically measured over weeks to months, and the biggest driver remains well-designed progressive loading. Any added tool should be viewed as supportive—not a replacement for rehab mechanics.
Conclusion
BPC-157 is most commonly discussed for tendon repair and recovery support, but when you zoom in on what does bpc 157 do to the brain, the honest answer is that direct, human, brain-specific effects aren’t clearly established in clinical practice. Reports may reflect systemic recovery changes, pain modulation, sleep differences, or indirect signaling—not necessarily a direct “brain action.”
Next step: If you’re considering BPC-157 for tendon recovery, start by locking in a tendon rehab plan you can execute consistently for 4–6 weeks and track both tendon function and brain-adjacent outcomes (sleep, mood, focus) separately so you can identify what’s actually changing.
Discussion