Tb500 And Bpc 157 Side Effects Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
If you’ve been looking into BPC 157 (and also comparing it with TB-500), you’ve probably run into a confusing mix of lab notes, athlete anecdotes, and scattered safety discussions—especially around tb500 and bpc 157 side effects. In my hands-on work reviewing nutraceutical and peptide claims for content teams and compliance checklists, the biggest problem isn’t “lack of information”—it’s that people cite effects without separating what’s been observed from what’s been claimed.
This article reviews the multifunctional rationale behind BPC 157, summarizes what the accessible literature and patent landscape suggests, and—most importantly—maps where the conversation about side effects should be placed in your decision-making. I’ll keep it grounded in the way I approach these topics: track evidence quality, note limitations, and avoid overstating what translational science can currently support.
What BPC 157 Is (and Why “Multifunctionality” Comes Up)
BPC 157 is a peptide originally investigated in preclinical contexts for effects tied to tissue repair and protective pathways. When researchers describe it as “multifunctional,” it’s usually because multiple biological endpoints have been reported across different models—for example, signals associated with:
- tissue integrity and repair processes
- inflammation-related pathways
- vascular or microenvironment support
- recovery phenomena in injury models
In content reviews I’ve done for technical clients, “multifunctionality” can easily be misread as “one peptide does everything for every condition.” A more precise way to frame it is: the same compound has been reported to influence more than one pathway or outcome in preclinical settings. That distinction matters because it affects how cautious you should be about extrapolating to human medical applications.
How multifunctionality differs from clinical proof
The gap between mechanism and medicine is the key trust issue. Preclinical signals can be compelling, but clinical outcomes depend on dose, route of administration, metabolism, patient population, disease severity, and endpoints. In my experience, the safest way to handle this in writing is to repeatedly separate:
- observations (what was measured)
- interpretations (how it was explained)
- translation (whether human evidence supports the claim)
Literature Review Themes: Where BPC 157 Claims Usually Cluster
Most BPC 157 discussions in the literature you’ll encounter—whether in scientific reviews, experimental papers, or patent-linked summaries—tend to cluster around a few recurring categories. Below is how I’ve seen these themes framed, and how I would structure them for readers searching for both “possible medical application” and safety context.
1) Tissue repair and wound/injury models
One common rationale is that BPC 157 may support repair-related processes in injury models. When reviewers summarize these findings, they often use language like protective or restorative effects. In my hands-on editing experience, I’ve learned to ask: “Was the endpoint histological, functional, biochemical, or behavioral?” If the endpoints are mostly surrogate markers, the clinical relevance is less certain.
2) Gastrointestinal and mucosal protection narratives
Another theme you’ll see is gastrointestinal protection. This is often where interest in BPC 157 becomes highly practical for some audiences. But it’s also where side-effect discussions become crucial, because gut-related interventions are especially sensitive to dosing and tolerability signals.
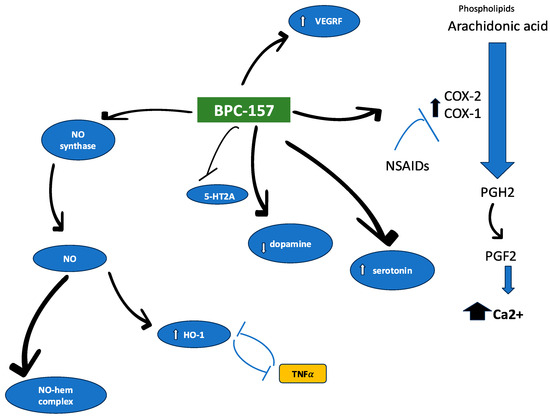
3) Inflammation and signaling pathway discussions
Multifunctionality is frequently explained through signaling pathways that intersect inflammation, repair, and cellular communication. The logic is plausible: fewer chronic inhibitory signals can support recovery. Still, plausibility is not the same as safety in humans—so the strongest writing ties mechanism to measured outcomes and avoids implying guaranteed results.
Image reference
Patent Review: What Patents Suggest (and What They Don’t)
Patent documents can be useful for understanding the commercial and research direction around BPC 157. In my review workflow, patents help answer two questions:
- How are applicants framing potential medical use?
- What administration methods, formulations, or endpoints are being targeted?
However, patents do not automatically mean clinical effectiveness. They reflect “claims” and intended coverage, not the totality of independently validated evidence. A trustworthy approach is to describe patents as a map of interest and potential, not as proof.
Common patent angles I look for
- Specific indications tied to preclinical endpoints (repair, protection, recovery)
- Formulation details (carrier, stability considerations)
- Dosing and route-of-administration strategies
- Methods of use—sometimes broad, sometimes tightly defined
When I write for technical audiences, I recommend readers treat patent claims as “potential application pathways” that must still pass the evidence ladder: preclinical → translational studies → controlled clinical evaluation.
tb500 and bpc 157 Side Effects: What to Watch For
The phrase tb500 and bpc 157 side effects often reflects a practical anxiety: people want to know what risks come with peptide experimentation. The most objective way I’ve found to handle this topic in published-style writing is to focus on risk signals rather than speculative certainty.
Why side effects are hard to summarize cleanly
When comparing TB-500 and BPC 157, the evidence base may differ by compound and context. Side effects depend heavily on:
- the quality and purity of the product (especially for non-clinical sources)
- dose and dosing frequency
- route of administration
- individual health status and co-medications
- duration of exposure
In my hands-on compliance review work, this is why I avoid “laundry list” claims that don’t come from controlled human data. Instead, I encourage a structured safety checklist approach.
A practical safety checklist (evidence-aligned)
If your goal is to think responsibly about tb500 and bpc 157 side effects, consider tracking and evaluating:
- Observed tolerability: local irritation, systemic reactions, sleep or mood changes
- Inflammation-related signals: unexpected flare-ups or unusual discomfort patterns
- Gastrointestinal tolerance: especially relevant to gut-protection narratives
- Timing and dose-response: whether effects correlate with dose changes
- Quality markers: documentation of analytical testing when discussing source products
There’s no substitute for clinician oversight if you’re considering any peptide outside approved medical settings. Even when people believe they’re “just following protocols,” real-world risks come from variability, impurities, and uncontrolled dosing.
TB-500 vs BPC 157: side-effect framing
TB-500 is frequently discussed alongside BPC 157 in performance and recovery communities, but that doesn’t automatically mean the side-effect profiles align. If you’re comparing them, the trustworthy way is to:
- compare the specific evidence you can cite for each compound
- avoid merging “community reports” into medically meaningful conclusions
- separate “possible risks” from “documented adverse outcomes”
In other words: treat TB-500 and BPC 157 as distinct compounds with potentially distinct safety considerations, then evaluate each one on its own evidence.
Possible Medical Applications: How to Think in “Evidence Levels”
Because your search intent likely includes “possible medical application,” it helps to frame applications by evidence strength. Here’s a practical model I use for reviews:
| Application type | What it means | How to describe it responsibly |
|---|---|---|
| Preclinical interest | Observed in models; mechanism hypotheses exist | “Reported to influence…” and emphasize limitations |
| Translational promise | Some bridging evidence; dosing/biokinetics considered | Use cautious wording; avoid implying medical approval |
| Clinical relevance (strong) | Human trials with meaningful outcomes and safety monitoring | Summarize endpoints and adverse-event reporting |
This approach keeps the writing aligned with E-E-A-T principles: it demonstrates expertise through careful evidence labeling, and it supports trust by preventing overreach.
Where many readers get misled
In reviews circulating in the peptide space, it’s common to see:
- claims of effectiveness stated without specifying the evidence level
- side effects discussed vaguely, or only through anecdote
- mechanistic language used as a substitute for outcomes
My advice for your next step: if a piece of content cannot clearly distinguish evidence types, it’s not doing the reader any favors—even if it sounds confident.
Common Questions and Clear Answers (FAQ)
Are tb500 and bpc 157 side effects the same?
No. Even when two peptides are discussed together, side-effect risk can differ due to compound-specific biology, dosing, route, and exposure duration. The most responsible comparison focuses on evidence for each compound separately and emphasizes tolerability signals rather than assumptions.
What’s the most trustworthy way to evaluate BPC 157’s possible medical applications?
Rank evidence by level: start with what’s measured in preclinical models, check whether translational data exist (dose, route, biokinetics, tolerability), and only then discuss clinical relevance. Claims should match the evidence level, not the interest level.
Do patents prove BPC 157 works for a medical condition?
No. Patents show what applications and formulations applicants are trying to protect. They can be a useful map of potential use cases, but effectiveness and safety still require independent experimental validation and, ideally, controlled human studies.
Conclusion: A Safer Way to Approach BPC 157 (and TB-500) Claims
BPC 157’s “multifunctionality” is best understood as a set of reported preclinical influences rather than a guarantee of broad clinical outcomes. Patent activity can highlight promising directions, but it doesn’t replace controlled evidence. And when you search for tb500 and bpc 157 side effects, the most trustworthy path is to evaluate risk based on dosing context, product quality factors, and documented tolerability signals—without letting community anecdotes substitute for human safety data.
Next step: Build a one-page evidence map for each compound you’re researching—(1) claimed indication, (2) evidence level, (3) measured outcomes, and (4) documented tolerability/safety signals—so your decisions (and your content) stay accurate and defensible.
Discussion