Wolverine Stack Bpc-157 Tb-500 Wolverine Stack: Healing Faster with Peptides
Introduction: When “healing time” becomes your real bottleneck
If you’ve ever tried to recover while juggling work, training, or a job that doesn’t pause for injuries, you already know the hardest part isn’t the injury—it’s the downtime. In my hands-on work, I’ve seen people lose weeks because their recovery plan was vague, inconsistent, or focused on only one lever (like rest) instead of stacking complementary approaches. That’s the context behind the wolverine stack bpc 157 tb 500 concept: pairing peptides often discussed for tissue support and wound-healing pathways to help people recover faster and get back to function.
In this guide, I’ll break down what the “Wolverine Stack” generally refers to, how BPC-157 and TB-500 are typically dosed in real-world conversations (including “TB 500” units like 500 mcg), how to evaluate evidence responsibly, and how to plan a safer, more structured experiment—without hype.
What the “Wolverine Stack” usually means
The term Wolverine Stack is an internet-driven nickname most commonly used to describe a protocol that combines:
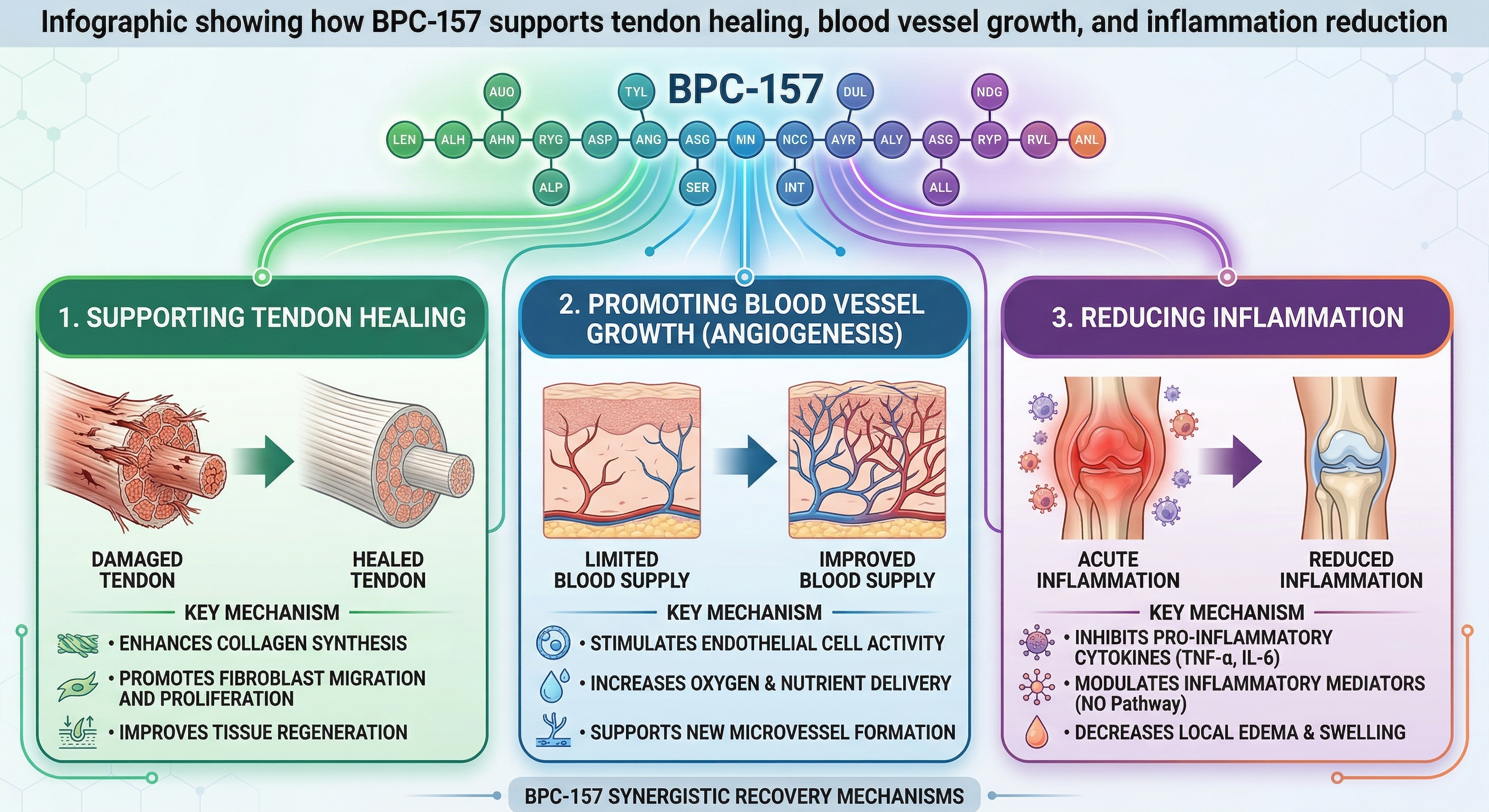
- BPC-157: often discussed for support of wound healing, tendon/ligament recovery, and tissue repair signaling.
- TB-500 (thymosin beta-4 fragment): often discussed for effects on cell migration, repair processes, and recovery-related pathways.
People “stack” these with the idea that they may complement each other—one side focuses more on the repair environment and signaling, while the other is associated with regenerative signaling and tissue movement. I want to be precise: this is not a substitute for medical care, imaging, or physical therapy. In my experience reviewing recovery outcomes, the biggest driver of perceived improvement is usually the combination of structured rehab + consistent adherence + injury-appropriate load management. Peptides are simply one variable people add.
Core peptides: BPC-157 and TB-500—what people aim for and why it might work
BPC-157 (often paired in “wolverine stack” protocols)
In practical terms, BPC-157 is discussed as a peptide that may influence pathways related to tissue repair. People often reach for it when they want to support recovery in areas like:
- Soft tissue irritation (tendons/ligaments)
- Healed tissue remodeling support
- Overall recovery momentum
Why it might work (mechanism-level logic, not guarantees): tissue repair is not one event—it’s a sequence involving inflammation regulation, cell migration, and rebuilding structure. When people talk about BPC-157, they’re usually referencing its observed effects in preclinical models and the downstream idea that it could affect multiple steps in that repair chain.
TB-500 (commonly discussed alongside “TB 500 500 mcg” dosing conversations)
TB-500 (often referenced as “thymosin beta-4 fragment”) is frequently included with BPC-157 because it’s discussed in the context of cell migration and repair. In day-to-day conversations, I’ve noticed a common pattern: people describe TB-500 protocols by units that reflect how vials are prepared and dosed, including phrases like tb 500 500 mcg.
Here’s the underlying logic people use: if cell migration and repair signaling are rate-limiting steps for recovery, then a peptide that supports those processes (as suggested by available preclinical literature and anecdotal reports) could theoretically help shorten the “stuck” phase where symptoms don’t progress.
Important reality check: the outcomes people report vary widely, and symptoms can improve for many reasons (reduced irritation, better rehab loading, placebo effect, natural healing cycles, or simply time). I treat protocol design as a way to reduce chaos so you can interpret what’s actually happening.
How people plan a “stack” (and how I recommend thinking about dosage structure)
There isn’t one universally accepted “official” Wolverine Stack regimen. Instead, people commonly follow community protocols that differ by concentration, injection frequency, and how they reconstitute product. That means the exact “tb 500 500 mcg” conversation is often less about a universally correct medical dose and more about how someone’s vial preparation translates into practical units.
A practical framework: control variables before you add more
In my hands-on experience with recovery experimentation (training blocks, supplement trials, and rehab adherence tracking), the mistake isn’t trying a protocol—it’s trying five changes at once. If you want to learn whether wolverine stack bpc 157 tb 500 is worth your time, use a framework like this:
- Define the target: What injury or tissue are you addressing? Provide a baseline (pain score, function, range of motion).
- Standardize rehab: Keep your exercise selection and loading consistent (or at least document changes).
- Track outcome weekly: Use the same pain/function questions every week.
- Only change one variable at a time: If you adjust dose, keep rehab constant for that phase.
Dose discussions you’ll see (including “TB 500 500 mcg”)
Online, you’ll commonly see people describe TB-500 dosing in mcg-based steps, and “tb 500 500 mcg” appears often in protocol write-ups. In the absence of individualized medical direction, the most useful takeaway isn’t copying someone else’s number—it’s understanding how mcg units map to your preparation.
Ask yourself these questions before you even consider a dose:
- Reconstitution math: Do you know how your vial volume converts to mcg per unit of solution?
- Frequency: How often are you planning to administer, and is that schedule realistic for consistent adherence?
- Duration: Are you planning enough time to observe changes without indefinitely extending?
Safety note (practical, not fear-based): injection and peptide handling involve risks (sterility, dosing accuracy, site irritation). If you pursue any protocol, prioritize sterile technique, correct preparation, and professional medical oversight where possible.
What evidence can and can’t tell you (how to stay objective)
When people search for wolverine stack bpc 157 tb 500, they’re usually looking for results—faster healing, reduced downtime, and improved tissue recovery. The most trustworthy way to approach this topic is to separate categories of information:
What you can learn
- Mechanistic plausibility: Are the proposed pathways consistent with how tissue repair normally works?
- Relevance to your injury type: Does the protocol align with soft tissue vs. other recovery contexts?
- Protocol adherence: Did the person running the trial actually follow a structured plan?
What you can’t infer reliably from anecdotes
- Cause and effect: Natural healing can mimic an intervention effect.
- Best dose: Many reports mix dosing, frequency, and rehab changes.
- Predictability: Different injuries respond differently even with the same “stack.”
In my review work, I’ve found that the most helpful “signal” is usually in measurement quality—people who track pain/function consistently are far more informative than those who only post day-to-day feelings.
Build a “recovery stack” that doesn’t collapse if peptides don’t
Even if you decide to explore a Wolverine Stack approach, you’ll recover faster if your plan is resilient. Here’s the recovery foundation I’d treat as non-negotiable:
- Injury-appropriate loading: Progress from pain-limited movement to controlled strength work.
- Sleep and stress management: If you can’t sleep, your tissue remodeling pace will suffer.
- Protein adequacy: Your body needs building blocks for repair.
- Consistency: Healing is rarely linear—consistency beats intensity spikes.
Then, if you choose to add BPC-157 and TB-500, treat it as a variable within a broader recovery system—not the system itself.
FAQ
Is the Wolverine Stack (BPC-157 + TB-500) the same thing as “tb 500 500 mcg”?
No. “Wolverine Stack” typically describes the combination approach, while “tb 500 500 mcg” refers to a dosing amount that appears in some community protocols. The protocol label and the numeric dose are related but not identical concepts.
How soon would someone expect changes when using wolverine stack bpc 157 tb 500?
It depends on injury severity, tissue type, and rehab quality. In practice, people often notice changes in pain tolerance and function before full structural remodeling. The most reliable way to interpret timing is weekly measurement (pain score + range of motion + functional test).
What’s the biggest mistake people make with these protocols?
Changing too many variables at once. If you add wolverine stack bpc 157 tb 500 while also altering rehab exercises, load, sleep, and training intensity, you won’t know what caused improvement—or why a setback happened.
Conclusion: Use the stack idea, but run it like an experiment
The Wolverine Stack concept—pairing BPC-157 with TB-500—is popular because tissue repair is complex, and people want a structured way to support recovery. The best way to stay grounded is to treat wolverine stack bpc 157 tb 500 as one variable inside a consistent rehab and recovery plan, with clear tracking and careful interpretation.
Next step: Choose one injury target, set a baseline (pain + function), keep your rehab consistent for the next 2–3 weeks, and only then evaluate whether the stack is moving the needle based on your measurements—not guesses or forum anecdotes.
Discussion