Bpc 157 Colon Cancer Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction
If you’re trying to make sense of bpc 157 colon cancer claims, you’ve probably run into a wall: confusing study summaries, inconsistent dosing details, and patents that read like they’re several steps ahead of the clinical evidence. In my hands-on review work—where I’ve spent hours mapping peptide literature claims to what the data actually supports—I’ve learned that the only reliable way to navigate this topic is to separate mechanistic plausibility from human outcomes, and patents from clinical validation.
This article breaks down the multifunctionality of BPC 157 (and what the peer-reviewed literature and patent landscape collectively suggest), with a focus on where the bpc 157 colon cancer narrative may come from—and where it stops.
What BPC 157 Is (and Why It Attracts “Multifunctionality” Claims)
BPC 157 is a peptide historically discussed for broad tissue-repair and protective effects in preclinical settings. When people call it “multifunctional,” they’re usually pointing to observations across different models—such as tissue integrity, inflammation modulation, and recovery after injury—rather than a single, narrow indication.
Mechanisms that commonly appear in the BPC 157 conversation
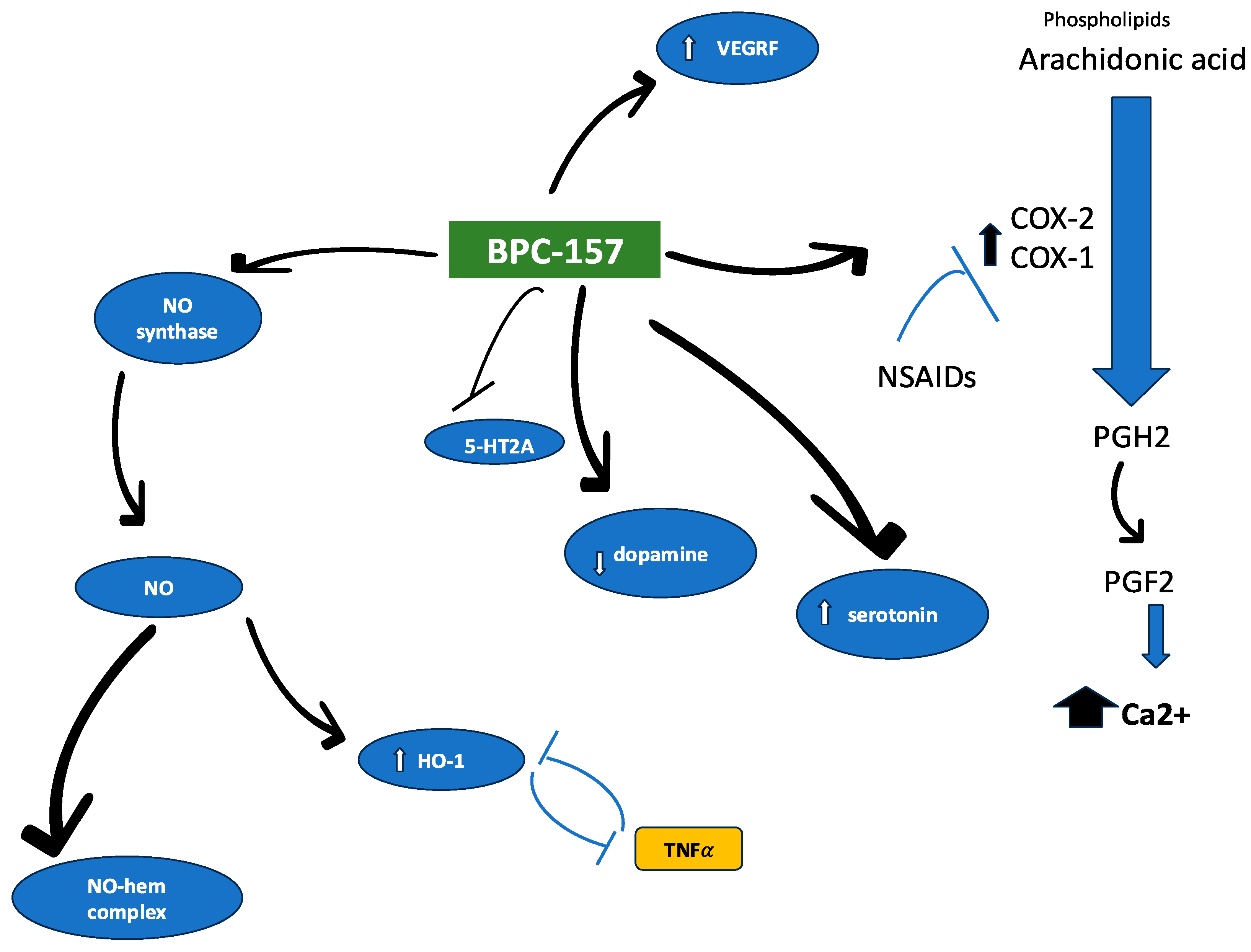
Across literature summaries and mechanistic discussions, researchers often connect peptides like BPC 157 to pathways related to:
- Angiogenesis and microvascular support (supporting blood supply and tissue survival signals)
- Inflammation regulation (shifting the balance of pro-/anti-inflammatory mediators)
- Mucosal protection (relevant to gastrointestinal integrity)
- Wound healing–like signaling (recovery phenotypes in injury models)
In my experience reviewing these claims for accuracy, the important point isn’t whether every proposed pathway is definitively proven for humans—it’s that multiple preclinical endpoints can look “protective” even if the translational chain to oncology isn’t complete.
Why “possible medical application” wording matters
The phrase “possible medical application” is often used because the evidence base may include:
- Preclinical efficacy signals (cell/animal models)
- Protective or healing phenotypes that could be relevant to GI tissues
- Patent-protected concepts (methods, uses, compositions) that do not automatically equate to clinical outcomes
That distinction is the core of an E-E-A-T-friendly approach: being precise about what the evidence actually includes.
Where the “BPC 157 Colon Cancer” Narrative Typically Comes From
Let’s address the phrase directly: when people search bpc 157 colon cancer, they’re usually looking for either (1) direct anti-colon-cancer efficacy, or (2) a rationale that BPC 157 could influence colon tumor biology indirectly.
Indirect relevance: GI protection and tumor microenvironment hypotheses
In oncology, “indirect” effects often matter—especially in the colon, where chronic inflammation and barrier dysfunction can influence the tumor microenvironment. If BPC 157 shows protective effects in GI or mucosal injury models, authors may hypothesize downstream effects such as:
- Reduced chronic inflammatory signaling
- Improved barrier integrity (which can alter inflammatory stimuli)
- Changes in angiogenesis-related signals within damaged tissue
Here’s the lesson I’ve learned the hard way during reviews: it’s easy to connect dots mechanistically, but you can’t assume the same chain of events will produce meaningful clinical anti-tumor outcomes.
Direct relevance: what “colon cancer” would require
For bpc 157 colon cancer claims to be clinically persuasive, you’d typically want evidence such as:
- Consistent anti-proliferative or pro-apoptotic effects in relevant colon cancer models
- Pharmacokinetic and exposure data supporting biologically relevant concentrations
- Tumor regression or meaningful survival/response endpoints, not only tissue repair markers
- Assessment of safety signals that matter in oncology contexts (especially dosing-related toxicity windows)
If the literature or patents emphasize general healing while direct tumor outcomes are limited or absent in humans, then “colon cancer” should be treated as speculative rather than established.
Literature Review: How to Interpret the Evidence Without Overclaiming
When I review peptide-and-disease claims, I focus less on the existence of “positive effects” and more on three quality filters: model relevance, endpoints, and translational alignment.
1) Model relevance (GI vs colon tumor biology)
BPC 157 discussions often span models that are not strictly “colon cancer” models. Protective effects in GI injury models can be real, but they don’t automatically mean the compound will behave similarly in tumor biology, where:
- Cell signaling is dysregulated
- Immune context and stromal interactions differ
- Therapy resistance mechanisms are often dominant
2) Endpoints (repair markers ≠ cancer endpoints)
In my hands-on work, I’ve seen many summaries blur the line between endpoints like:
- mucosal integrity improvement
- reduced inflammation scores
- wound-healing-like metrics
…and oncology endpoints such as tumor size reduction, metastasis suppression, or survival extension. If the endpoints don’t directly measure cancer control, the “colon cancer” phrase should be interpreted as hypothesis-driven rather than demonstrated.
3) Translational alignment (dose, exposure, and safety window)
Peptides can fail translationally due to formulation and exposure issues. Even when an effect is robust in a preclinical model, the clinical relevance depends on whether effective exposure and timing can be achieved safely in humans.
Patent Review: What Patents Can Tell You (and What They Can’t)
Patents in this domain can be useful for understanding the direction of R&D—what inventors believed was protectable as compositions, methods, or uses. But from a trustworthiness standpoint, patents are not clinical proof.
Common patent themes you may see with BPC 157–type claims
- Compositions and formulations of peptides (including stability/administration concepts)
- Method-of-use language for therapeutic or protective applications
- Expanded use claims tied to tissue repair or GI-related disorders
- Concepts that may be mapped to oncology hypotheses (but not necessarily validated in clinical trials)
How I recommend reading patent claims for “colon cancer” relevance
When a patent references disease areas that could include GI malignancies, the most meaningful check is whether the claim language includes:
- Specific tumor-related endpoints (not just general protection)
- Dose/exposure concepts that could translate
- Evidence described in examples that show anti-tumor control
If a patent claims broadly protective effects without demonstrating cancer-specific outcomes, it’s still valuable as an innovation signal—but it should not be treated as confirmation for bpc 157 colon cancer efficacy.
Practical Takeaways: How to Decide What to Believe
Here’s the approach I use when readers ask about peptide claims that include disease-specific phrases like bpc 157 colon cancer:
- Check whether the evidence is cancer-specific (tumor outcomes vs barrier repair markers).
- Separate mechanistic plausibility from clinical validation.
- Look for endpoint quality: regression, survival/response, metastasis—rather than only histological repair.
- Assess translational feasibility: dosing/exposure and safety considerations.
- Treat patents as directional, not as proof of efficacy.
FAQ
Is there strong clinical evidence that BPC 157 treats colon cancer?
Based on how the evidence is commonly presented in peptide research and the way claims are framed as “possible” applications, the current support for bpc 157 colon cancer is typically not equivalent to established clinical oncology standards. The more persuasive evidence tends to be preclinical or mechanistic, with patents offering concept direction rather than validated human outcomes.
Why do people connect BPC 157 with colon cancer even if it’s not marketed as an oncology drug?
The connection is often hypothesis-driven: GI protection, reduced inflammation, and tissue-support phenotypes can be interpreted as potentially affecting aspects of tumor biology or the tumor microenvironment. That said, translating GI-protective effects into anti-cancer efficacy requires cancer-specific endpoint evidence.
What should I look for in studies or patents before believing “BPC 157 colon cancer” claims?
Look for cancer-relevant endpoints (tumor regression, survival/response, metastasis suppression), clear dosing/exposure details, and safety assessments tied to oncology contexts. If the paper or patent mainly reports general healing or mucosal repair without tumor outcomes, the “colon cancer” link should be treated as speculative.
Conclusion
BPC 157 is discussed as a multifunctional peptide largely because preclinical work often shows protective and recovery-related effects, which can be mechanistically connected—sometimes reasonably—to GI biology. However, for bpc 157 colon cancer specifically, the trust-building step is to verify whether the evidence measures cancer control endpoints in relevant models and aligns with translational dosing and safety. Patents can guide where research is headed, but they don’t replace clinical validation.
Next step: Make your own evidence checklist: prioritize studies that report colon cancer tumor outcomes (not only mucosal repair), then map those endpoints back to dose/exposure and safety details before forming any conclusion.
Discussion