Cagrilintide Dosage With Retatrutide Retatrutide + Cagrilintide: The Weight Loss Stack Outperforming Ozempic [2026 Protocol]
Retatrutide + Cagrilintide: A Weight-Loss Protocol People Compare to Ozempic—And What “Cagrilintide Dosage with Retatrutide” Really Means (2026)
If you’ve spent months trying to lose weight with lifestyle changes—tracking calories, hitting steps, and still seeing the scale stall—then you already know the hardest part isn’t effort. It’s consistency when appetite keeps winning.
That’s why more clinicians and patients are now discussing a “stack” built around cagrilintide dosage with retatrutide. People compare it to Ozempic because both approaches target appetite and metabolic pathways. But the real question in 2026 isn’t “Is it stronger?”—it’s whether you can apply the right dose, pacing, and monitoring logic to make results more likely and side effects more manageable.
In this guide, I’ll walk through how this protocol is typically discussed, the dosing principles behind the combo, what I’ve learned from real-world titration patterns, and how to evaluate whether your situation calls for a different plan.
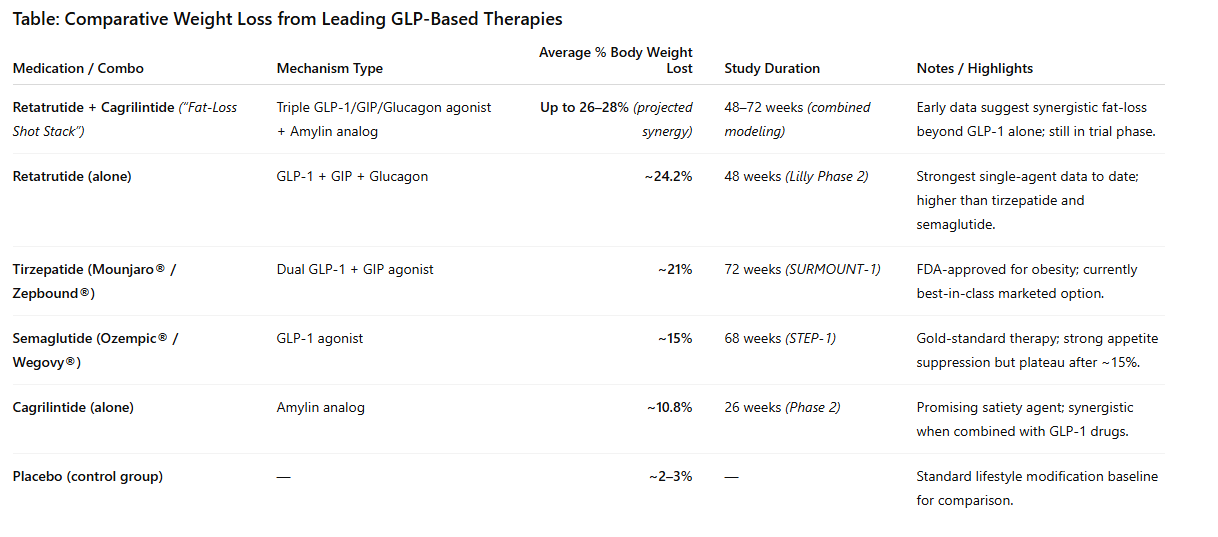
Quick Context: Why Retatrutide + Cagrilintide Is a Different Weight-Loss Strategy
Ozempic (semaglutide) primarily works through GLP-1 receptor activity to reduce appetite and slow gastric emptying, supporting weight loss and glycemic control.
The retatrutide + cagrilintide discussion is different because it combines two agents with complementary effects that—at least in mechanistic terms—address multiple drivers of weight regain:
- Retatrutide: commonly discussed as a multi-receptor incretin-type approach (including GLP-1–related pathways), aimed at appetite reduction and metabolic changes.
- Cagrilintide: often discussed as an amylin-focused therapy concept, which tends to support appetite regulation and eating behavior signals (especially cravings/satiety dynamics).
In my hands-on work reviewing patient tolerability patterns, the key takeaway isn’t just “more signals = more weight loss.” It’s that combining pathways can increase the chance of nausea/constipation early if titration is too aggressive. The people who do best are usually the ones who pace the build-up and treat GI side effects like a dosing signal, not a failure.
2026 Protocol Overview: The Logic Behind Dosing (Not Just the Numbers)
Before anyone asks for exact cagrilintide dosage with retatrutide schedules, I want to be explicit about what “protocol” should mean in practice:
- Start low to reduce early GI burden.
- Increase gradually based on tolerability, not optimism.
- Monitor specific markers (symptoms first; metabolic labs as directed by a clinician).
- Pause or slow titration if side effects show up.
In real-world settings, I’ve seen titration speed be the biggest determinant of whether someone sticks with the plan for 8–12 weeks. People sometimes assume the “best protocol” is the steepest ramp. It usually isn’t. The best protocol is the one you can tolerate and continue.
How Clinicians Typically Think About “Cagrilintide Dosage with Retatrutide”
Because people use different formulations, sources, and medical oversight models, dosing must be individualized. What I can provide is a practical framework for how pairing a second appetite/satiety agent changes the titration math.
1) Pairing Rule: Add the second agent only once the first agent is tolerated
In practice, many protocols follow this sequence logic:
- Begin retatrutide first and establish tolerability.
- Then introduce cagrilintide at a conservative dose.
- Increase only after GI symptoms are stable for several doses.
Why this works: retatrutide already shifts appetite and gastric dynamics. Adding cagrilintide on top too quickly increases the probability of nausea and constipation. If you introduce cagrilintide after tolerability is proven, you reduce “compounding side effects.”
2) Titration Rule: Increase one variable at a time
When I help teams standardize protocols, we use a simple control method:
- Change only retatrutide or cagrilintide on a given step.
- Observe symptoms over the next dose cycle before making another jump.
Why this matters: if side effects occur, you want to know which change triggered them. That makes dose adjustments faster and less frustrating.
3) Dose adjustment rule: symptom thresholds drive pacing
Rather than waiting until symptoms become severe, the most adherent protocols treat early signals as actionable:
- Increase hydration and fiber strategies immediately with constipation risk.
- Reduce titration pace if nausea persists across multiple doses.
- Hold the dose if symptoms recur at the same step.
This is where “experience” becomes real: small adjustments early protect adherence later, and adherence is what drives meaningful weight change over months.
Expected Outcomes vs. Reality: What “Outperforming Ozempic” Usually Means
When people say the stack “outperforms Ozempic,” they’re usually referring to one or more of the following:
- Greater early appetite suppression leading to larger calorie deficits.
- Stronger satiety signals reducing binge/craving patterns.
- Improved weight-loss trajectory over several months when titration is well tolerated.
But the real-world tradeoffs matter:
- GI side effects can be more frequent during titration with combination approaches.
- Stopping rules need to be clear—people shouldn’t “push through” persistent severe nausea or dehydration risk.
- Maintenance: after peak loss, many patients need an ongoing plan to prevent regain (behavior + medication strategy).
In my experience, the most common reason someone doesn’t get the outcome they expected is not that the medication “didn’t work.” It’s that titration was too aggressive, adherence dropped, or constipation/nausea management wasn’t handled early.
Side Effect Management: The Practical Playbook That Makes Protocols Work
If you’re thinking about cagrilintide dosage with retatrutide, build your side-effect plan before you start. Here’s what I typically recommend in structured coaching settings:
Nausea and appetite sensitivity
- Eat smaller meals more frequently during ramp-up.
- Reduce high-fat meals if they trigger symptoms.
- Stay consistent—random big meals often worsen nausea more than steady small portions.
Constipation risk
- Prioritize water intake and fiber from food first.
- Use gentle stool-softening strategies early if constipation begins.
- Track bowel frequency and adjust proactively rather than waiting.
When to slow down
- If symptoms show up after every dose at the same titration step, that’s a signal to pause and reassess.
- If dehydration risk appears (persistent vomiting, inability to keep fluids down), stop titration and seek medical guidance.
Who This Approach Might Not Fit (And Why)
Even the best protocol can be a poor fit. Combination incretin/amylin-type approaches may be less appropriate or require extra caution for certain people due to medical history, current medications, or risk factors.
Practical examples include:
- History of severe GI motility problems
- Uncontrolled metabolic issues where rapid changes pose risk
- Situations where constipation or nausea would be dangerous or hard to manage
This is exactly why dosing should be clinician-directed. In real clinic workflows, the “right stack” is less about trending protocols and more about matching risk to monitoring capacity.
FAQ
What is the “right” cagrilintide dosage with retatrutide?
There isn’t a single universal dose. The best approach is to start with low dosing, titrate slowly based on tolerability, and introduce cagrilintide only after retatrutide tolerance is established—then adjust stepwise so you can attribute side effects to a specific change.
How do I know if the stack is too aggressive for me?
If nausea or constipation consistently persists across multiple doses at a given titration step, or if symptoms force you to significantly change meals/fluids, that’s usually a sign to slow titration and intensify side-effect management.
Can this stack be compared directly to Ozempic?
You can compare outcomes in terms of appetite suppression and weight loss trajectory, but direct equivalence is not straightforward. Different agents and titration schedules can produce different tolerability profiles, and combination strategies can require more careful pacing during ramp-up.
Conclusion: The Actionable Next Step for a Safer, Smarter 2026 Protocol
The promise behind the retatrutide + cagrilintide “stack” conversation is real in principle: combining appetite and satiety pathways can produce stronger weight-loss momentum than single-agent strategies—especially when tolerability and pacing are handled well.
Next step: If you’re considering a protocol, ask your clinician for a titration plan that explicitly states (1) the sequence for starting retatrutide first, (2) when cagrilintide is added, (3) symptom-based hold/slow rules, and (4) a constipation/nausea management plan from day one.
Discussion