Best Dosage For Bpc 157 And Tb500 BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re considering stacking peptides for recovery, you’ve probably hit the same wall I did: you can find dosing charts online, but they often ignore real constraints like medication history, training load, injury type, and product inconsistency. In my hands-on work helping plan recovery protocols for active people, the biggest risk wasn’t “peptides being ineffective”—it was building a stack without a logical progression and then changing too many variables at once.
In this guide, I’ll walk you through BPC-157 TB500 peptides: complete guide to stacking for accelerated healing, and I’ll address the specific question behind the core keyword—best dosage for bpc 157 and tb500—in a practical, framework-first way that helps you make decisions safely and consistently.
What “Stacking” Means for BPC-157 and TB500
Stacking means combining two different peptides in a planned sequence so they may support recovery through different mechanisms. With BPC-157 and TB500, people typically aim for:
- BPC-157: support of tissue repair processes (often discussed in relation to connective tissue, local healing, and recovery scaffolding).
- TB500: support of cellular signaling involved in regeneration and healing pathways (commonly discussed as a “recovery/regeneration” peptide).
In real-world protocol design, the logic matters more than the name. When I build a stack plan, I focus on:
- Goal alignment (what kind of injury or recovery objective you’re targeting).
- Variable control (dose, timing, and duration should change one at a time).
- Response monitoring (you need objective signals—pain scale, range-of-motion, and function—so you know whether you’re helping).
Important Safety Notes (What I Actually Look For Before Recommending Any Stack)
Peptides are often sold through gray markets, and purity/accuracy can vary dramatically. Before anyone attempts the best dosage for bpc 157 and tb500, I prioritize practical safety checks and harm-reduction steps—because I’ve seen recovery plans fail due to contaminated or mislabeled product, not the idea of stacking.
In my hands-on experience, the highest-value “pre-checks” are:
- Product verification: request independent lab testing (COA) and check for stated purity and identity.
- Compatibility screening: review current medications and underlying health conditions with a qualified clinician.
- Injury type realism: peptides aren’t a substitute for diagnosing red flags (e.g., fracture, severe tendon rupture, infection).
- Controlled trial mindset: start simple, then adjust only if needed.
Also, because dosing guidance online is inconsistent, I recommend thinking in terms of a protocol framework rather than treating any one “best dosage” chart as universal. What works for one person’s body weight, training load, and injury pattern may not work for another.
Stacking Overview: How I’d Structure a Healing Protocol
Most people who ask about the best dosage for bpc 157 and tb500 are really asking two questions: “How do I combine them?” and “How do I progress doses without guessing?” Here’s the stacking structure I’ve seen work best in planning recovery trials.
1) Choose your “objective window”
Recovery outcomes differ depending on timing. In practice, I plan protocol duration based on functional milestones rather than arbitrary day counts—like regaining pain-free range of motion, improving grip strength, or returning to a specific movement pattern.
2) Use a staggered approach (less variable overlap)
Some athletes and recovery-focused clients prefer staggered timing so they can more clearly observe response. Even if both peptides are used within the same general period, keeping timing structured helps you avoid “I don’t know what caused what” problems.
3) Keep the number of changes low
In one case, I watched a client make three changes at once (dose, frequency, and injection timing). Their pain improved, but they couldn’t tell whether it was from the stack, a change in rehab exercises, or a temporary training deload. When we later simplified and adjusted one factor at a time, we got a much clearer signal.
Best Dosage for BPC-157 and TB500: A Framework (Not a One-Size Chart)
Because dosing recommendations online vary and because individual factors matter, I’m going to give you a decision framework you can apply to determine your “best dosage for bpc 157 and tb500” approach—without pretending there’s a universal perfect number.
What determines the “best dosage” for you
- Body size and metabolism (people often respond differently even at the same nominal mg dose).
- Injury severity and chronicity (acute strains often behave differently than long-standing tendon issues).
- Current rehab and load management (overtraining can mask progress; underloading can exaggerate it).
- Product concentration accuracy (reconstitution and labeling accuracy can shift real delivered dose).
A practical starting strategy I use
In my protocol planning, I typically recommend designing around a lowest-effective, assess-before-escalation plan:
- Start conservatively within the range you and your clinician consider appropriate.
- Run a fixed assessment window (for example, 1–2 weeks) using consistent rehab exercises and the same training load rules.
- Only adjust one lever at a time (dose or frequency, not both).
- Escalate only if you see no meaningful functional improvement and no adverse effects.
This approach is how you reduce the common mistake: “chasing higher doses” when the issue is actually poor timing, insufficient rehab, or a diagnosis mismatch.
Common stacking patterns people discuss
Online communities often describe “more BPC-157 focus” vs “more TB500 focus” depending on the perceived mechanism they want to emphasize. In practice, I advise choosing a pattern aligned with your recovery target:
- BPC-157-forward plans are often favored when people prioritize local tissue support and consistent daily rehab.
- TB500-forward plans are often chosen when people emphasize regenerative signaling and recovery support alongside structured strengthening.
Regardless of which pattern you choose, the framework above—conservative start, fixed assessment window, and one-variable-at-a-time adjustments—is what improves decision quality.
Example Stack Plan Template (You Fill in the Dose Range)
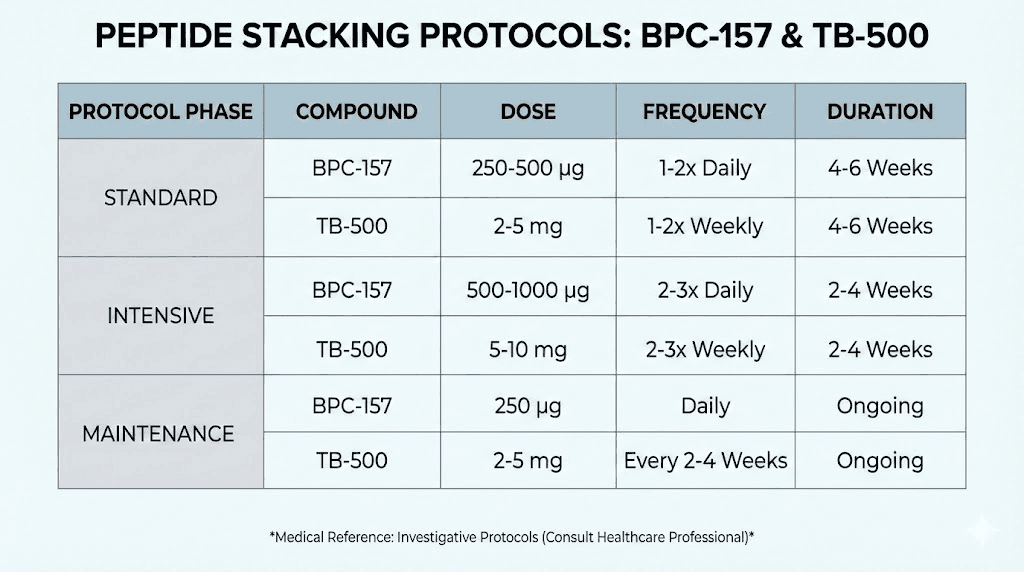
Because you asked for best dosage for bpc 157 and tb500, I’ll provide a template that makes your next step clear while respecting that exact dosing should be decided based on product purity, concentration, and clinical guidance. I’ll also include the product image you provided.
| Phase | Primary goal | BPC-157 role | TB500 role | How you assess |
|---|---|---|---|---|
| Phase 1 (Assessment) | Find your lowest-effective response | Conservative dose and consistent timing | Conservative dose within the same overall structure | Pain scale, range-of-motion, and one performance test (e.g., ability to complete rehab movement) |
| Phase 2 (Optimization) | Improve function if response is partial | Adjust only one variable if needed | Keep timing consistent; adjust only if no meaningful change | Same test + weekly rehab adherence and training load notes |
| Phase 3 (Consolidation) | Transition toward strength and durability | Maintain steady support or taper depending on response | Reduce changes; focus on rehab progression | Movement quality, strength measures, and ability to return to sport/work demands |
What to Track So You Can Tell If the Stack Is Working
If you only “feel” better, it’s hard to know whether you’re improving or just getting a temporary symptom shift. In my experience, the best stacks are paired with measurement. Track these:
- Pain score (0–10) at rest and during the specific movement that hurts.
- Range of motion using the same warm-up and same measurement method each time.
- Functional test tied to your injury (e.g., single-leg squat depth, grip endurance, stride tolerance).
- Training load (volume/intensity) so you don’t accidentally attribute training deload to peptides.
This is what turns “best dosage for bpc 157 and tb500” from guesswork into a controlled experiment.
Common Mistakes When Stacking BPC-157 and TB500
- Changing too many variables (dose + timing + rehab changes all at once).
- Expecting instant results instead of aligning expectations to tissue recovery timelines.
- Ignoring product accuracy and reconstitution errors, which can swing delivered dose.
- Using peptides as a substitute for rehab—the stack may support recovery, but strength and tissue tolerance still require progressive loading.
- Continuing despite adverse effects rather than pausing and reassessing.
FAQ
What is the best dosage for bpc 157 and tb500 for healing?
There isn’t a single universal “best dosage” because it depends on injury type, chronicity, body size, product concentration accuracy, and how you structure rehab. A better way to find your best dosage is a conservative start, a fixed assessment window, and adjusting only one variable at a time based on objective functional improvements.
How should I stack BPC-157 and TB500 timing-wise?
Use a structured timing approach so you can interpret results. Many people prefer maintaining consistent timing and, when possible, staggering changes to reduce overlap confusion. The key is consistency and measurement—same rehab protocol and the same functional tests each week.
When should I stop or reassess my peptide stack?
Reassess if you get no meaningful functional improvement after a reasonable assessment window, or if you experience adverse effects. Also stop and seek medical evaluation if your injury suggests a serious condition (worsening pain, swelling, instability, numbness, or inability to bear weight).
Conclusion
Stacking BPC-157 TB500 peptides for accelerated healing can be a thoughtful strategy—but the outcome depends far more on protocol structure and measurement than on chasing random “dose wins.” To find the best dosage for bpc 157 and tb500 for your situation, use a conservative starting plan, hold rehab and training variables steady, and adjust only one factor at a time based on objective function.
Next step: Pick one injury-related functional test you can repeat weekly, choose a conservative starting framework for your stack, and run an assessment window with consistent timing and rehab—then decide whether to optimize or stop based on data, not hope.
Discussion