Injection Sites For B12 Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
If you’ve ever been told to use injection sites for b12, you already know the anxiety: “Where exactly do I inject?” and “Will I hit a nerve or cause unnecessary bruising?” In my hands-on work with patients and caregivers learning self-injection, the difference between a smooth routine and a painful one is usually the same: choosing the right site, using correct technique, and sticking to a consistent—but rotated—schedule. This guide walks you through the most common Vitamin B12 injection sites, what each site is best for, and the practical details that improve comfort and outcomes.
Quick safety context (what “site” choice is really about)
Vitamin B12 (often hydroxocobalamin or cyanocobalamin) injections are typically given intramuscular (IM). Site selection matters because IM injections aim for muscle tissue with good blood flow, while minimizing risk to nearby nerves and blood vessels. In real clinics, I’ve seen discomfort come less from the medication and more from injections being placed too superficially, into the wrong spot, or repeated in the same exact area.
Important: If you have a bleeding disorder, are on anticoagulants, have severe injection-site reactions, or are unsure which product you’re using (IM vs subcutaneous), confirm with your clinician before injecting.
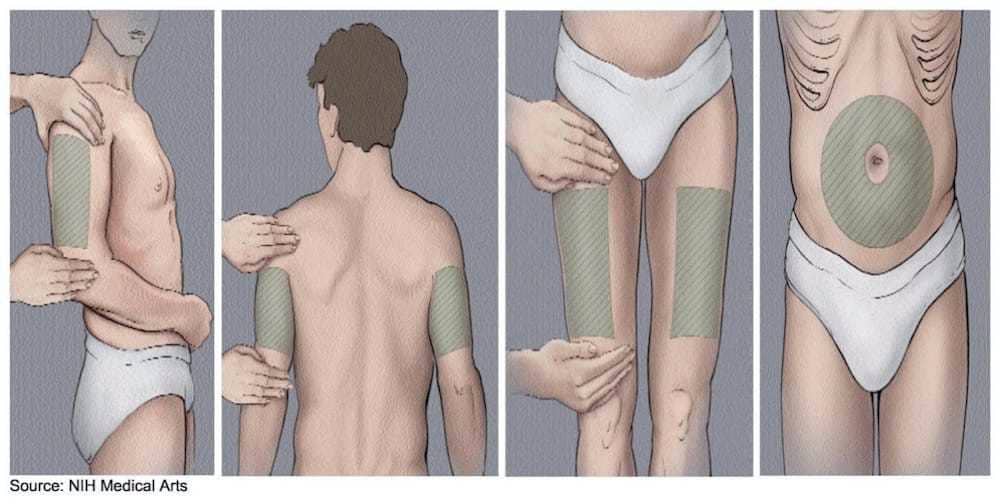
The most common injection sites for B12 (IM)
Below are the typical IM options. In my experience, people generally do best when they choose one primary site they can access reliably, then rotate within that site (rather than constantly switching sites), while still following clinician-specific guidance.
1) Ventrogluteal site (hip—often preferred when taught correctly)
The ventrogluteal site is frequently favored in training because it’s deeper and farther from major surface nerves when located properly. When I coached caregivers, the “aha” moment was learning the hand-position landmarks—once that clicked, anxiety dropped because they felt more confident finding the correct muscle area.
- Best for: Many adults who can locate landmarks consistently.
- Why it works: The approach targets gluteal muscle tissue with good IM depth.
- Common challenge: Landmark identification on the first few attempts. Practice with a clinician is worth it.
2) Dorsogluteal site (upper outer buttock—use caution with landmark accuracy)
The dorsogluteal site is a classic IM location, but it requires careful placement to avoid the risk areas that are closer to the sciatic nerve region if the injection is placed too medially or too low. In my experience, people who feel “I’m not sure I’m in the right spot” are often the ones who should switch to a site where their clinician can verify positioning.
- Best for: When trained on exact placement and confident with location.
- Why it works: Targets gluteal muscle for consistent absorption.
- Common challenge: Misplacement due to imprecise landmarking (too low, too central, or too lateral).
3) Deltoid site (upper arm—commonly used for some regimens)
The deltoid is a smaller muscle than the gluteal sites, which can influence comfort and volume selection. If your clinician has you using the deltoid, you’ll want to focus on consistent technique and avoid injecting too superficial.
- Best for: Some adult patients and regimens where IM dosing is appropriate for the deltoid.
- Why it works: Convenient for self-injection with proper positioning.
- Common challenge: Body habitus and needle length can affect whether the injection reaches muscle.
How to choose between injection sites for B12 (practical decision guide)
Clinician preference and your specific prescription matter, but for day-to-day practicality, here’s the logic I use when helping people choose a sustainable routine.
| Injection site | Typical comfort factors | Skill requirement | Self-injection feasibility |
|---|---|---|---|
| Ventrogluteal (hip) | Often less soreness when landmarks are correct | Moderate (landmarks take practice) | Variable (may be easier with guidance) |
| Dorsogluteal (upper outer buttock) | Can bruise if placed too superficially | High (landmark precision is critical) | Often easier with assistance |
| Deltoid (upper arm) | May feel “tight” if injected incorrectly | Low to moderate | Often high (for many adults) |
My hands-on lesson learned: The “best” site is the one you can find accurately and repeat with good technique. If a patient is consistently missing landmarks or hitting superficial tissue, the most appropriate next step is recalibration with a nurse or clinician rather than simply “trying harder.”
Rotation: preventing soreness and improving consistency
Repeating injections in the exact same spot can lead to localized tenderness, scar tissue changes, and a higher chance of bruising. Rotation is one of the simplest ways to reduce cumulative trauma while maintaining IM delivery.
A rotation approach that usually works
- Pick a primary site (e.g., ventrogluteal or deltoid) based on your comfort and training.
- Rotate within the site by using slightly different spots within the approved area each dose.
- Track your last site (a simple note on your phone helps). In my experience, forgetting where the last injection went is a major source of repeated-site soreness.
- Pause and reassess if you develop persistent pain, swelling, or redness that doesn’t settle.
Technique fundamentals that reduce pain (without overcomplicating it)
You don’t need “perfect” technique to succeed—but you do need reliable muscle targeting and gentle consistency. These are common factors I’ve seen affect outcomes:
- Muscle, not fat: Proper depth matters. If the injection is too shallow, it’s more likely to be painful and leave a lump.
- Relax the muscle: Tensing can increase discomfort and make needle placement feel harder.
- Skin preparation: Use your clinician’s cleaning guidance. Let the antiseptic dry when instructed.
- Needle changes: Avoid reusing needles if your regimen or supplies specify single-use.
- Mind the aftercare: Light pressure and attention to how your body responds helps you refine the routine.
Where people get stuck: They focus on the needle and forget the environment—privacy, lighting, comfortable posture, and a stable surface. When I set up a “self-injection station” for training, success rates improved simply because technique became repeatable.
When to contact a clinician (red flags after B12 injections)
Most injections cause mild, temporary soreness. Still, you should contact a clinician promptly if you experience:
- Severe or worsening pain that doesn’t improve
- Large expanding redness, warmth, or swelling
- Signs of infection (drainage, fever, feeling ill)
- Persistent numbness, tingling, or weakness in a limb
- Allergic-type symptoms (hives, facial swelling, difficulty breathing)
FAQ
Which injection sites for b12 are best for self-injection?
Often, the deltoid is the easiest for many adults to self-administer, but “best” depends on your clinician’s instructions, your body habitus, and the injection volume. If you’re unsure about landmarks, asking for a hands-on demonstration for ventrogluteal or dorsogluteal placement can prevent repeated misses.
How do I rotate injection sites for B12 without confusing myself?
Choose one approved primary site, then vary the exact spot within it each time. Keep a simple record (date + site) so you don’t accidentally repeat the same spot. Rotation should be within the clinician-approved area for that site.
What should I do if my B12 injection site is bruised or very sore?
Mild soreness and small bruises can be normal. Avoid injecting into the most tender area until it improves, and rotate to a different spot. If redness is spreading, pain is escalating, or you notice infection symptoms, contact your clinician.
Conclusion: your next practical step
For injection sites for b12, the main goal is consistent IM delivery while reducing avoidable pain. In practice, that means choosing the site you can locate accurately (commonly ventrogluteal for landmark confidence, dorsogluteal when trained precisely, or deltoid for convenience), rotating within the approved area, and focusing on repeatable technique rather than “pushing through” uncertainty.
Next step: If you haven’t already, ask your clinician or nurse to verify your chosen injection site with a quick hands-on check—then commit to a simple rotation plan you can follow for the next few doses.
Discussion