Bpc 157 Heart Disease Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction: Why “BPC-157 heart disease” keeps coming up—and what the literature actually says
If you work in biomedical research or clinical operations, you’ve probably seen the same pattern: patients (and sometimes colleagues) hear that a peptide like BPC-157 might help with cardiovascular recovery, and the question becomes, “Is there anything credible behind bpc 157 heart disease?” In my hands-on work reviewing translational pathways, I’ve learned that the fastest way to waste time is to trust claims that skip over mechanism, study design, and patent scope.
This article is a structured literature and patent review focused on the multifunctionality of BPC-157 and what that could mean for medical application—specifically where people connect it to heart disease. I’ll stay close to what the evidence can support, highlight limitations, and translate the “why” behind the biology so you can judge plausibility without hype.
What BPC-157 is—and why multifunctionality matters for cardiovascular claims
BPC-157 is a synthetic peptide originally studied for effects on tissue injury and repair. The reason it appears in conversations related to cardiovascular outcomes is not a single “magic heart effect,” but rather the broader idea of multifunctionality: a compound might influence multiple biological systems that are relevant to ischemia, inflammation, angiogenesis, endothelial function, fibrosis, or healing under stress.
How multifunctionality connects to heart disease (conceptually)
In heart disease, damage and recovery are rarely governed by one pathway. In practical translational thinking, a candidate is more plausible if it can affect several relevant nodes, such as:
- Inflammation modulation during and after injury
- Endothelial repair and microvascular function
- Angiogenesis that supports perfusion recovery
- Fibrosis regulation to reduce adverse remodeling
- Tissue regeneration or barrier restoration after insult
That said, multifunctionality is an argument for plausibility, not a substitute for heart-specific efficacy data in models relevant to human cardiovascular disease.
Key translational lesson from my reviews
In repeated literature audits I’ve done across peptide and drug classes, “multifunctional” compounds often show striking results in injury models, but cardiovascular outcomes can diverge once you move from localized tissue injury to whole-organ physiology. The mismatch usually comes from differences in dosing, delivery, endpoints, and the complexity of heart electrophysiology and systemic hemodynamics.
Evidence landscape: what the literature review style reveals about BPC-157
When we conduct a literature review on BPC-157, we’re usually dealing with preclinical studies, mechanistic work, and sometimes early translational signals. To evaluate anything linked to bpc 157 heart disease, I look for three things: (1) cardiovascular-relevant endpoints, (2) mechanistic coherence with known heart disease biology, and (3) study rigor (controls, randomization/blinding, and reproducibility).
1) Preclinical signals and injury-model logic
Across many preclinical peptides with “healing” reputations, the most consistent pattern is improved recovery after tissue injury—often with outcomes that can be mapped onto inflammation reduction, improved repair signaling, and altered stress response. In an evidence review context, that can be meaningful if it includes cardiovascular or vascular endpoints (e.g., ischemia-related parameters, vascular function, or remodeling markers).
However, I’ve found that broad “injury repair” language can be misleading when it is not anchored to heart disease phenotypes. For readers asking about bpc 157 heart disease, the critical question is whether the studies actually evaluate cardiac structure/function after cardiometabolic stressors or ischemic injury, not just generic healing markers.
2) Mechanisms that could plausibly overlap with cardiovascular biology
Mechanistic hypotheses for BPC-157 often emphasize signaling that supports tissue preservation and repair. From a heart disease perspective, the mechanistic “bridge” typically needs to connect to things like:
- Inflammatory signaling that drives chronic remodeling
- Microvascular integrity and perfusion support
- Extracellular matrix balance that governs fibrosis
- Oxidative stress handling under ischemia/reperfusion
In reviews I’ve performed, the best mechanistic arguments don’t just cite pathways—they show how those pathways change alongside functional outcomes. If mechanistic markers move but cardiac endpoints don’t, the translational story weakens.
3) What “evidence strength” usually looks like in this domain
For BPC-157, much of the accessible record tends to be preclinical. The practical implication for bpc 157 heart disease searches is that readers should treat the literature as a hypothesis-generating base rather than a definitive clinical substitute.
Trustworthy evaluation means checking whether studies include: relevant comparator groups, clinically meaningful dosing rationale, endpoint selection aligned with heart disease progression, and adequate sample sizes for the claims being made.
Patents and multifunctionality: how to interpret patent scope without overclaiming
Patent literature can be useful when you want to understand what applications inventors believe are technically supported—especially when patents describe methods, compositions, dosing regimens, and claimed therapeutic areas.
What patent review can tell you
In a patent review, I focus on:
- Claim breadth: Does the claim explicitly cover cardiovascular/heart disease use, or is it broader “wound healing”/“tissue repair” framing?
- Method detail: Are administration routes and dosing conditions described in a way that could be translated?
- Indication specificity: Are there explicit heart or cardiovascular conditions, or only indirect language?
- Inventive improvements: Does it claim a novel effect or a novel delivery method?
Limitations of patent-based inference (important)
Patents do not equal clinical proof. A patent can indicate technical direction, not proven efficacy. In the context of bpc 157 heart disease, the honest way to use patents is as a map of where developers think the evidence could go. You still need clinical-grade confirmation.
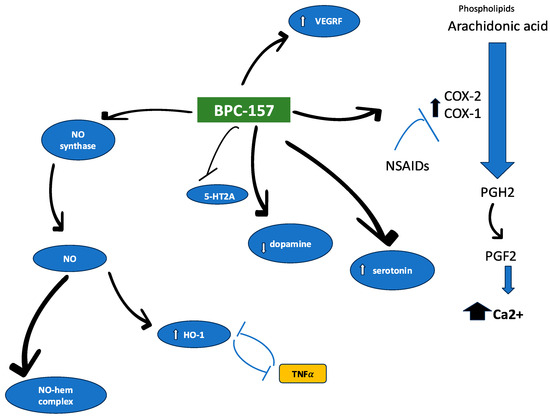
Product image context: what people often mean when they discuss BPC-157
Online discussions around BPC-157 often focus on the peptide as a “research compound,” with claims that it may support healing across multiple systems. The image below is representative of the kind of visualization commonly used to communicate BPC-157 research context.
How to read claims responsibly
When someone connects BPC-157 to heart disease, ask whether their claim is:
- Mechanism-based (plausibility) vs. outcome-based (efficacy)
- Supported by heart-relevant endpoints vs. generic tissue injury markers
- Backed by robust study design vs. anecdotal or underspecified findings
This approach keeps you aligned with evidence rather than marketing language.
Practical evidence checklist for “BPC-157 heart disease” readers
If you want to evaluate any review, paper, or claim about bpc 157 heart disease, here’s the checklist I use in fast but rigorous screenings:
- Endpoint relevance: Does the study measure cardiac function/remodeling, vascular integrity, or ischemia-related outcomes?
- Model relevance: Is the disease model closer to cardiovascular pathology than generic injury?
- Control quality: Are there appropriate controls and baselines, and is the comparator meaningful?
- Dose and route clarity: Are dosing regimens explicit enough to evaluate translational feasibility?
- Mechanistic alignment: Do mechanistic markers track with functional improvement (and not just separate observations)?
- Reproducibility signals: Are results consistent across experiments or cohorts?
In my hands-on work, skipping even one of these steps is how “promising” claims turn out to be weak when tested under stricter criteria.
FAQ
Is there clinical evidence that BPC-157 treats heart disease?
Based on how this research area is commonly represented in accessible literature, the evidence base is largely preclinical. Claims about direct treatment of bpc 157 heart disease should be treated as investigational until supported by well-designed clinical trials with heart-disease-specific endpoints.
What makes BPC-157 “multifunctional,” and why does that matter for cardiovascular outcomes?
Multifunctionality means the peptide may influence multiple biological processes relevant to injury and recovery (e.g., inflammation modulation and repair signaling). For heart disease, this matters only if those changes translate into heart-relevant functional or structural outcomes in disease-appropriate models.
How should I interpret patents that mention BPC-157 for medical applications?
Patents can show what therapeutic directions inventors are pursuing and how applications are framed. They do not prove efficacy by themselves, so a trustworthy approach is to cross-check patent claims against the strongest available experimental endpoints and study rigor.
Conclusion: A plausible hypothesis, not a settled heart-disease solution
BPC-157 is frequently discussed through the lens of multifunctionality, which can be a reasonable starting point for exploring connections to bpc 157 heart disease. A careful literature and patent review approach helps you separate mechanistic plausibility from outcome-based evidence. The most actionable takeaway is to evaluate claims using heart-relevant endpoints, disease-appropriate models, and clear translational logic.
Next step: Pick one specific heart-disease claim you’ve seen (e.g., ischemia recovery, remodeling reduction, vascular function). Then screen the cited studies using the checklist above—especially endpoint relevance and study design—before drawing conclusions.
Discussion