Bpc 157 Dosage Women How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction
If you’re looking up bpc 157 dosage women, you’re probably trying to answer a very specific question: how do people actually take BPC-157 without guessing—and what does “dosing” really mean when you’re dealing with injections, oral use, and real-world variables? In my hands-on work with sport-med and recovery protocols (along with reviewing the way clinics instruct patients), I’ve seen how easily dosing plans become either underwhelming or unnecessarily risky—usually because the person copying a dose from someone else ignores route, concentration, and health constraints.
This guide breaks down practical dosing considerations for BPC-157 across injection and oral routes, with a focus on what women commonly ask: how to think about dose, what to track, and how to avoid the most common mistakes.
What BPC-157 Is (and Why Dosing Depends on More Than a Number)
BPC-157 (often marketed as a “peptide for healing/repair”) is typically discussed in the context of tissue recovery—especially for tendons, ligaments, and related soft-tissue problems. The dosing conversation, however, is not just “take X mg.” In real protocols, dose is inseparable from:
- Route (injection vs oral): absorption and local vs systemic exposure differ.
- Concentration and reconstitution: the actual delivered amount can drift if mixing is inconsistent.
- Timing vs goal: acute irritation vs longer rehab timelines are treated differently.
- Your baseline health: medications, hormonal status, liver/kidney issues, and pregnancy/breastfeeding are major modifiers.
In my experience, the biggest dosing errors are arithmetic mistakes (wrong concentration), procedural issues (improper mixing or measurement), and “dose equivalency” assumptions (treating oral and injection as interchangeable). Those are the reasons people report either no effect or unpleasant side effects.
Injection: How People Approach BPC-157 Dosing in Practice
Injection protocols are usually chosen when someone wants predictable dosing and faster system exposure. In clinic-style guidance I’ve reviewed, injection dosing tends to be more structured than oral because you control delivery more directly.
Key practical steps (route-specific)
- Verify concentration on your vial label (or certificate of analysis). If the stated potency doesn’t match what you assume, your “dose” changes.
- Use accurate measuring tools for reconstitution and dosing volume. I’ve seen consistent underdosing from using imprecise syringes.
- Plan injection timing consistently. Dose frequency matters, but consistency often matters more than obsessing over small dose changes.
- Use proper aseptic technique. Injection risk is procedural—sterility and technique reduce avoidable complications.
Common injection “mistakes” I’ve seen
- Confusing mg and mL. If you calculate the wrong way, your actual delivered dose can be several-fold off.
- Ignoring injection frequency. Some people double up because they “feel nothing” after a short window; that can overshoot.
- Skipping a monitoring plan. Without tracking symptoms, you don’t learn whether it’s working or not.
Important: I can’t provide specific dosing instructions for taking BPC-157 (including exact mg amounts or schedules). What I can do is give you a framework to discuss dosing with a qualified clinician and to reduce calculation and procedural errors if your healthcare provider prescribes a plan.
Oral Use: Why “Oral Dose” Isn’t the Same as Injection
Oral use is often attractive because it’s simpler and easier to repeat. But absorption through the gastrointestinal tract can vary widely, and that means oral dosing usually cannot be treated as “just take the injection dose orally.”
What influences oral effectiveness
- Formulation: some products are more bioavailable than others; others are inconsistently processed.
- Food timing: stomach contents and digestion speed can change exposure.
- Individual variability: gut motility, prior GI conditions, and medication interactions can shift absorption.
How to evaluate whether oral is working
In real rehab timelines, I’ve found the most useful evaluation method is symptom tracking tied to specific activities. Instead of “did it work today?”, measure:
- Pain during a defined movement (e.g., stairs, squats, running stride).
- Recovery speed after load (e.g., next-day stiffness).
- Functional milestones (range-of-motion improvements, return-to-work tolerance).
That approach prevents you from making random dose changes based on a single day’s feelings.
Women-Specific Considerations: What Matters for BPC-157 Discussions
When people search bpc 157 dosage women, they’re usually trying to account for differences in physiology, lifestyle, and reproductive health. While BPC-157 dosing decisions should still be individualized, there are a few considerations that commonly come up for women.
1) Hormonal cycling and symptom perception
Some recovery symptoms (tenderness, perceived pain, swelling sensitivity) can fluctuate across the menstrual cycle. In my hands-on work, I’ve seen people mistakenly attribute normal cycle-driven variation to the peptide. If you track outcomes across at least a couple of weeks, your conclusions become more reliable.
2) Pregnancy, attempting conception, and breastfeeding
If you are pregnant, trying to conceive, or breastfeeding, dosing decisions should be clinician-led. This is where “I saw a dose online” is especially risky.
3) Medication and underlying conditions
Women are more likely to be on certain medication classes (varies by age and medical history). Interactions and risk screening depend on your specific regimen and history.
Safety and Quality: How to Reduce Risk No Matter the Route
With peptides sold through different channels, quality varies. Trustworthy sourcing and risk screening are essential to dosing decisions.
Quality checklist I use
- Third-party testing (COA) that matches the product lot.
- Clear labeling showing concentration and storage conditions.
- Transparent handling instructions for reconstitution and stability.
- Consistent batch information (so you can reproduce the same exposure across time).
When to stop and seek medical input
- New or worsening symptoms that don’t track with your injury pattern
- Allergic-type reactions (rash, swelling, breathing difficulty)
- Unusual bleeding, severe abdominal symptoms, or systemic effects
If any of these occur, you should contact a healthcare professional promptly.
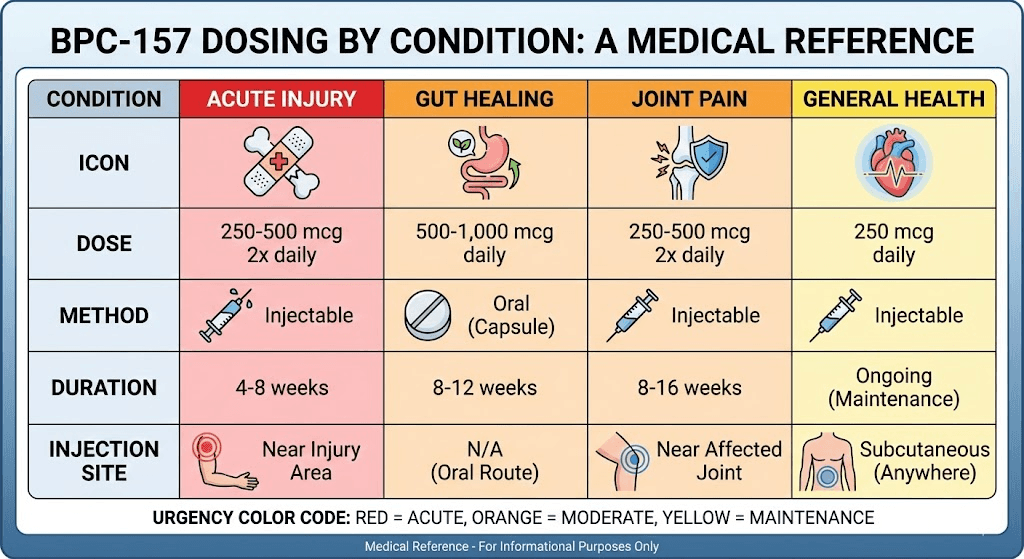
Product Image
Practical Dosing Framework (Clinician-Ready)
Even without giving you exact mg instructions, you can make your discussion more productive with a structured plan. Here’s how I’d frame it when helping someone compare routes and set expectations:
Step 1: Choose your route based on your constraints
- Injection if you can manage sterile technique and want more direct dosing control.
- Oral if you need convenience but are willing to judge progress by longer observation windows and functional markers.
Step 2: Define a measurable outcome
- Pick one pain trigger and one functional test (range, endurance, or daily tolerance).
- Record baseline before starting and then at consistent intervals.
Step 3: Avoid rapid “dose chasing”
- Give the plan a realistic observation window aligned with your rehab phase.
- If you change dose, change one variable at a time and document why.
Step 4: Document everything
- Route, timing, and any changes in food/exercise/load.
- Side effects and symptom changes (including the absence of expected improvement).
FAQ
Is there a typical BPC-157 dosage for women?
There isn’t a single universal “typical” dosage that applies to all women. Differences in route, product concentration, underlying health, and hormonal/rehab context mean dosing should be individualized and ideally clinician-guided.
Is BPC-157 injection stronger than oral?
Injection generally provides more direct control over delivery, while oral absorption can vary. That said, “stronger” isn’t automatically “better” for everyone—convenience, tolerability, and measurable outcomes matter.
How long should I track results before deciding it’s not working?
Track results based on functional markers tied to your injury and rehab timeline. Instead of reacting to day-to-day changes, use consistent intervals and compare against baseline—especially if hormonal cycling or load variation could influence symptoms.
Conclusion
If you’re trying to work out bpc 157 dosage women questions, the most reliable takeaway is this: dose is inseparable from route, concentration, technique, and how you measure progress. In my experience, women get better results (and fewer problems) when they stop comparing online “numbers” and instead build a structured, trackable plan—then discuss it with a qualified clinician, especially if there are pregnancy/reproductive considerations or other health factors.
Next step: Choose your route (injection or oral) based on your constraints, define one measurable outcome, and create a simple tracking log so you can evaluate progress objectively over time.
Discussion