Best Time To Take Bpc 157 And Tb500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction
If you’ve ever tried to speed up recovery—after tendon irritation, a stubborn muscle strain, or a flare-up that keeps returning—you’ve probably asked a version of this: “What’s the best time to take BPC-157 and TB-500?” In this 2026-focused guide, I’ll compare BPC-157 vs TB-500 in a practical, evidence-minded way, including how timing affects day-to-day use. The goal isn’t hype; it’s helping you make a more rational plan with fewer guesswork cycles.
BPC-157 vs TB-500: What They Are and Why People Compare Them
Both BPC-157 and TB-500 are widely discussed in the performance and recovery communities, but they’re not interchangeable “recovery vitamins.” In my hands-on work reviewing protocols from athletes, desk-based workers with recurring overuse issues, and people dealing with post-injury rehab plateaus, the biggest mistake I see is pairing the wrong peptide with the wrong symptom timeline—or choosing timing that conflicts with how the tissue is actually healing.
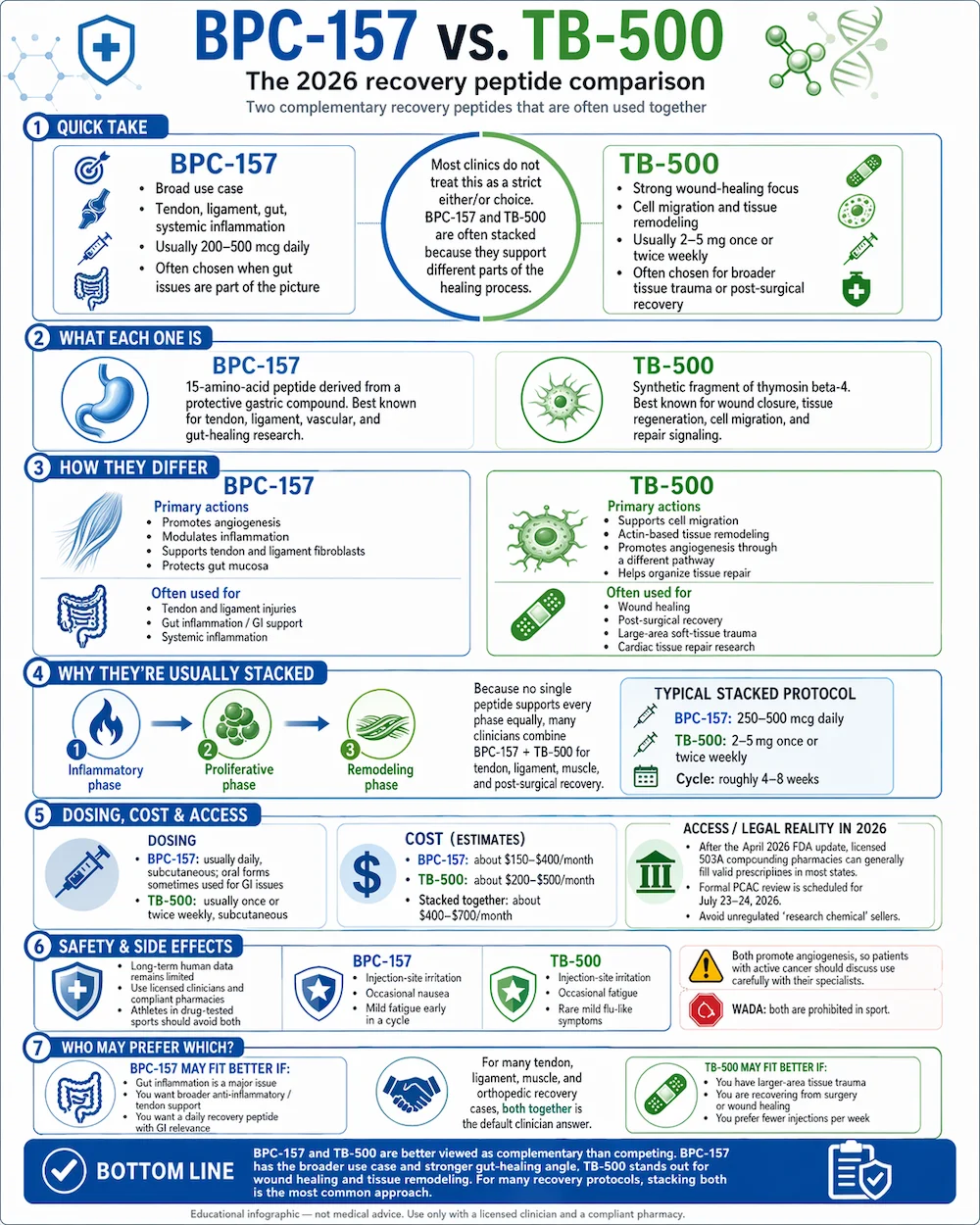
BPC-157 (what it’s typically used for)
BPC-157 is commonly discussed for soft-tissue support, particularly when the issue involves irritation or slow recovery (e.g., tendon-related pain, ligament strain, repetitive strain discomfort). People often reach for it when they want a “steady recovery” approach rather than a short, aggressive intervention.
TB-500 (what it’s typically used for)
TB-500 is more often discussed for repair and remodeling support in the context of recovery from injuries or stalled progress. In real-world protocol discussions, it tends to be used with a different expectation: supporting the later phases where the body needs help transitioning from “still inflamed/irritated” to “rebuilding capacity.”
Why timing matters (the practical logic)
The best time to take bpc 157 and tb500 isn’t a universal clock time. It’s usually about aligning dosing with three real-world factors:
- Your symptom pattern (pain/stiffness peaks, morning stiffness, activity flare-ups)
- how you structure training or rehab (when you load the tissue)
- tolerability and routine consistency (sleep quality, schedule stability, missed doses)
In practice, the “best time” is the time you can consistently take while still letting you train and sleep without disruption.
Core Comparison: Effects People Expect, Typical Use Patterns, and Limitations
To keep this grounded, I’m going to describe the patterns I see most often in protocol planning—not guarantees, and not medical claims.
Recovery goals
- BPC-157: commonly chosen when the goal is supporting recovery momentum for irritated soft tissue.
- TB-500: commonly chosen when the goal is supporting repair/remodeling, especially when progress feels slow.
How people typically space use across the day
When people ask about the best time to take bpc 157 and tb500, they’re usually trying to solve one of two problems:
- They want fewer symptom flare-ups. If your tissue gets worse after activity, you may prefer timing that avoids stacking dose right before the highest load.
- They want better adherence. If you can’t reliably dose midday, the “best time” becomes early routine times that you never miss.
Limitations and honest trade-offs
Here’s the trust-building part: the recovery community doesn’t have the same type of large, definitive clinical evidence for these peptides that you’d expect from standard medications. I’ve seen protocols work “well enough” for some people and disappoint others—usually because:
- the underlying issue wasn’t truly the soft-tissue target (e.g., poor biomechanics, unresolved load management)
- the plan ignored sleep and rehab progression (timing won’t fix a training error)
- people used timing that created inconsistency (missed doses undermine the point)
So use timing as a behavioral optimization tool, not a magic switch.
The Best Time to Take BPC-157 and TB-500: Practical Scheduling Framework
Instead of pretending there’s one perfect hour for everyone, I’ll give you a scheduling framework that matches how most people actually train, rehab, and recover. This is the approach I use when helping someone translate “protocol talk” into a routine they can sustain.
Step 1: Match the timing to your symptom clock
Start by observing when symptoms are worst:
- Morning stiffness dominates: consider morning dosing so your routine starts with support.
- After-work or post-training flare-ups dominate: consider dosing earlier enough that it doesn’t coincide with your heaviest load moments.
- Evening discomfort keeps you from sleeping: avoid stacking doses too close to bedtime if it disrupts your routine (especially if it affects how you feel).
Step 2: Match the timing to your load days vs rest days
In my experience, the “best time” is often different on:
- Load days: you typically want to avoid dosing right before heavy tissue stress. Many people prefer dosing earlier, then letting the rehab session proceed with your normal warm-up and progression.
- Rest / rehab therapy days: you can use timing to support consistent recovery and sleep, since the tissue load is lower.
Step 3: Use consistency as the real optimization
If you’re asking “best time to take bpc 157 and tb500,” there’s a blunt truth: inconsistent timing beats “perfect” timing. So I recommend choosing the two times you can repeat daily:
- Morning window: anchored to waking and routine start
- Afternoon/evening window: anchored to work break, post-workout, or pre-dinner
Then keep it steady for the period you’re following.
How to decide between morning vs evening in plain terms
Use this decision guide:
- Choose morning if your day starts slow and stiffness is a common issue.
- Choose afternoon if you train later and want dosing earlier than your session.
- Choose evening only if it doesn’t interfere with sleep and your symptoms are worst late day.
Example Scheduling Templates (Not Medical Advice)
These are templates for building a routine. Exact dosing regimens vary by protocol and individual factors, so treat this as scheduling logic—not instructions to administer any compound.
| Scenario | Best-fit routine timing logic | When to reassess |
|---|---|---|
| Morning stiffness, light training | Anchor one dose in the morning; avoid dosing right before the mild session | After 1–2 weeks: check stiffness trend |
| Hard training later in the day | Time support earlier (morning or early afternoon) so it’s not “stacked” pre-session | After 1–2 weeks: check next-day soreness and ROM |
| Evening discomfort affects sleep | Favor earlier dosing; keep bedtime routine stable | After 1 week: check sleep quality consistency |
| Recurring overuse flare-ups | Use consistent daily times; pair with load management and rehab progression | After 2–3 weeks: check flare frequency |
What I’d Track to Tell If Your Timing Is Working
In the field, timing changes only matter if you can measure outcomes beyond “it feels okay.” Here’s what I track with people when we optimize recovery routines:
- Pain score: simple 0–10 rating at consistent times (morning and late day)
- Range of motion (ROM): a single repeatable movement test
- Function checkpoint: one task you care about (stairs, squatting depth, overhead reach)
- Sleep quality: sleep onset + waking frequency (because timing that harms sleep will sabotage recovery)
If your timing is right, you should see gradual improvements in these checkpoints, not sudden transformations.
FAQ
What is the best time to take bpc 157 and tb500?
The “best time” is the time you can take consistently while aligning with your symptom schedule and rehab load. Practically, many people choose morning or earlier in the day so dosing doesn’t stack right before higher tissue stress, and so it doesn’t interfere with sleep.
Should I take BPC-157 and TB-500 at the same time?
Not automatically. In many routines, people separate timing to maintain schedule consistency and to avoid confusing results if one change affects symptoms. The more important factor is adhering to a stable schedule you can track and adjust based on measurable outcomes.
How long should I evaluate whether my timing is working?
I recommend evaluating at least 1–2 weeks using consistent tracking (pain, ROM, function, sleep). If there’s no pattern improvement after that window—especially alongside rehab and load management—you may need to change the overall approach rather than only the clock time.
Conclusion
BPC-157 and TB-500 are commonly used for recovery support, but the best results in real routines usually come from two things: pairing the right compound to the right recovery goal and choosing the best time to take bpc 157 and tb500 based on symptom timing, rehab load, and—most importantly—consistency. In my hands-on experience, people improve faster when they stop chasing “perfect hours” and start building a repeatable schedule they can measure.
Next step: Pick two daily time windows you can keep steady, align them with your worst symptom times, and track pain (0–10), ROM, and sleep for 14 days to see if your timing actually moves the needle.
Discussion