Cpt Code For Administration Of B12 Injection CPT Code 20610 Billing Guide
I’ve seen billing teams lose weeks of momentum—and sometimes cash—because they weren’t separating “what the clinician did” from “what the claim form should say.” The details matter, especially when the documentation crosses procedure boundaries. In this guide, I’ll walk you through a practical CPT code for administration of B12 injection workflow while also giving you the CPT Code 20610 Billing Guide framework for accuracy, coding logic, and claim-ready documentation.
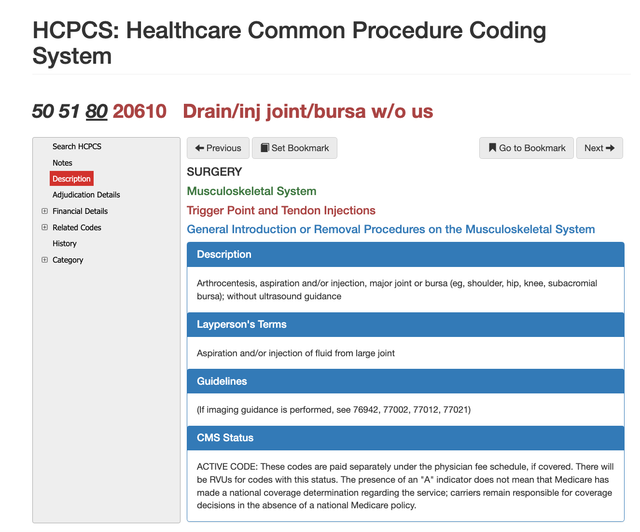
First, clarify what CPT 20610 is (and what it isn’t)
CPT 20610 is used for arthrocentesis (aspiration and/or injection) for the major joint or bursa. That wording is the anchor: 20610 is about a joint/bursa aspiration or injection—not about routine medication administration into the skin or muscle.
In my hands-on experience working through billing denials, the most common root cause is treating CPT selection like “any injection goes together.” It doesn’t. When a visit includes an injection, the coding depends on:
- Anatomic route (intra-articular vs. intramuscular vs. subcutaneous)
- Indication and purpose (diagnostic/therapeutic injection into a joint vs. medication administration)
- Documentation specificity (which joint/bursa, whether aspiration occurred, guidance used if applicable)
Key takeaway: If your goal is a CPT code for administration of b12 injection, you should not assume 20610 fits. Use 20610 only when the service documented truly matches “major joint or bursa” aspiration/injection.
CPT code for administration of B12 injection: where 20610 fits (and where it doesn’t)
For B12 injections, the clinician is typically administering cyanocobalamin (or another B12 preparation) intramuscularly (IM) or subcutaneously (SC). That is medication administration, not arthrocentesis of a major joint.
So how do you connect this to the CPT Code 20610 Billing Guide approach?
Use the “service-to-code mapping” checklist
- Injection location recorded? Example: “Left deltoid IM” or “Right arm SC.” If it’s skin/muscle, you’re outside the 20610 definition.
- Joint/bursa specified? Example: “Knee joint aspiration” or “Shoulder bursa injection.” If yes, 20610 becomes relevant.
- Aspiration documented? 20610 often implies aspiration and/or injection related to the joint/bursa—your note should reflect what was performed.
- Was this an immunization/therapeutic injection policy? Some offices follow internal workflows for common meds; still, the final CPT must match what happened clinically.
When you might see both billing threads in one encounter
It’s possible for a single visit to include:
- A B12 injection (IM/SC) for deficiency management, and
- A separate major joint/bursa aspiration/injection (where 20610 may apply).
In those cases, the claim should reflect the appropriate CPT(s) for each discrete service, supported by documentation that makes the distinction obvious.
CPT 20610 Billing Guide: what you need for clean claims
Below is the billing logic I’d use to prepare claims with fewer back-and-forths. Treat it like an internal checklist for accuracy and audit-readiness.
1) Document the joint/bursa precisely
Include:
- Which major joint or bursa (e.g., knee, shoulder, hip bursa)
- Laterality when relevant
- Whether aspiration occurred and any descriptive notes (e.g., fluid characteristics if your documentation standard includes it)
2) Confirm the “aspiration and/or injection” language matches the note
20610 is not just “an injection happened.” It’s injection/aspiration associated with a major joint/bursa. I’ve seen denials when clinicians documented a medication injection but did not clearly tie it to joint/bursa aspiration/injection as described in the CPT definition.
3) Check guidance, supplies, and modifier usage
Some payers have specific requirements for modifiers or documentation around technique (for example, guidance). I recommend you follow your payer contract rules and keep a consistent documentation template.
Practical lesson from the field: In my work, claims got cleaner when we standardized the note template fields—so “joint/bursa + laterality + aspiration/injection + any guidance” were always present. That reduced coding disputes because the coding decision was defensible.
4) Ensure you’re billing administration correctly alongside medication supply
If your encounter includes medication administration (like B12) and a joint/bursa procedure, you must avoid blending services. The CPT for the injection itself and any related supply/medication line items depend on your billing setup and payer rules.
Goal: Each line item should correspond to a clearly documented service.
Visual example: where “site + purpose” should be obvious
When charting supports coding, claims process faster. If you’re using imaging or a standardized procedure record, make sure the “what/where” fields are unambiguous.
Documentation details that usually matter in audits
- Procedure site (joint/bursa vs. muscle vs. skin)
- Procedure intent (therapeutic injection/aspiration vs. medication administration)
- Performance evidence (what was done during the encounter)
- Separateness of services (if multiple injections occurred)
Common pitfalls (and how to prevent them)
-
Pitfall: Billing 20610 for a B12 IM/SC injection.
Fix: Ensure B12 is documented as IM/SC medication administration; reserve 20610 for major joint/bursa aspiration/injection. -
Pitfall: “Injection” written in the note without specifying joint/bursa.
Fix: Require the note to name the major joint/bursa and whether aspiration occurred. -
Pitfall: Combining services so the coder can’t justify the CPT selection.
Fix: Keep each service discrete in the record (and in the claim lines).
FAQ
What is the CPT code for administration of B12 injection?
Typically, B12 administration is coded based on the route (intramuscular vs. subcutaneous) and payer rules. The CPT you use should match how the injection was administered and what the documentation supports—not a major joint/bursa arthrocentesis code.
When would CPT 20610 be appropriate in an encounter that also includes B12?
CPT 20610 is appropriate only if the chart documents an aspiration and/or injection into a major joint or bursa. B12 injection alone (IM/SC) does not meet that definition, so the services must be documented separately.
Why do claims for 20610 get denied most often?
Most denials stem from documentation not supporting the joint/bursa aspiration/injection definition, unclear site/route details, or coding that doesn’t align with what the clinician actually performed.
Conclusion: your next best step
If you want fewer denials, treat “injection” as a category—not a CPT answer. Use a simple mapping rule: document the route and site, then select the CPT that matches the exact clinical service. Your actionable next step: review your last 10 encounters that included a B12 injection and confirm the notes clearly separate IM/SC medication administration from any major joint/bursa aspiration/injection. Then align your claim line CPTs to those documented facts.
Discussion