Bpc-157 Human Trials BPC-157 and the Difference Between an Evidence Gap and a Cover-Up: What the entire human evidence base actually looks like, and the questions to ask next. — WellFounded
Introduction: When the “evidence” story feels fuzzy, what are you actually looking at?
If you’ve tried to understand bpc 157 human trials, you’ve probably run into a familiar problem: claims are loud, summaries are inconsistent, and the underlying evidence can feel like it’s being discussed without showing its shape. In my hands-on work reviewing clinical evidence for supplement–to–pharma narratives, the most frustrating moments aren’t the disagreement—they’re the missing transparency: outcomes, trial quality, sample sizes, and what exactly was (or wasn’t) evaluated.
This article explains how to tell the difference between an evidence gap and a cover-up when it comes to BPC-157. We’ll also walk through the questions you should ask next—so you can evaluate the human data more rigorously instead of relying on marketing storylines.
First, define the two competing narratives: evidence gap vs. cover-up
When people discuss BPC-157, they often imply one of two things:
- Evidence gap: trials exist—or at least plausible pathways exist—but the human database is limited, not yet large enough, or not measured with modern endpoints.
- Cover-up: researchers or companies allegedly suppressed meaningful human findings.
In practice, “cover-up” claims require stronger support than “we don’t yet have enough data.” In my experience, the quickest way to reduce confusion is to check whether the evidence that should be visible is actually visible in legitimate channels—protocols, publications, trial registries, conference abstracts, and—most importantly—what the published outcomes say.
What an evidence gap usually looks like
- Small number of human studies, often with heterogeneity (different dosing regimens, injury models, outcomes).
- Endpoints that may not match what clinicians care about (e.g., surrogate outcomes instead of function and long-term recovery).
- Quality limitations: unclear randomization, limited blinding, incomplete reporting, or underpowered sample sizes.
- Results that are mixed or preliminary, leading to cautious interpretation rather than definitive clinical adoption.
What a cover-up would need to explain
A “cover-up” theory would need to account for why multiple independent signals are missing. For example, if robust beneficial human outcomes exist, you’d expect:
- More frequent and consistent results across studies and sites.
- Clear reporting of effect sizes, adverse events, inclusion/exclusion criteria, and durability of outcomes.
- Evidence of research momentum: follow-up trials, registry entries aligned with publication timelines, and replication attempts.
I’ve reviewed enough translational areas to know that absence of evidence can mean many things—but “cover-up” is rarely the simplest explanation.
What to inspect in bpc 157 human trials (and what to ignore)
Let’s get concrete. When you’re assessing bpc 157 human trials, the goal isn’t to find a single headline claim—it’s to map the evidence. In my hands-on approach, I treat each study like a data problem: who was studied, what was measured, how it was measured, and how confidently you can infer causality.
1) Study design: do you have a causal signal?
Look for study types and features:
- Randomization (or strong allocation justification)
- Blinding of participants and/or assessors
- Control group (placebo, standard of care, or active comparator)
- Pre-specified endpoints (not only post-hoc “wins”)
Why this matters: for BPC-157–style narratives, expectation effects and natural recovery can be substantial. Without controls and careful assessment, positive anecdotes can inflate perceived efficacy.
2) Outcomes: what actually improved?
Ask whether studies measured outcomes that matter clinically:
- Time to functional recovery (not only symptom reports)
- Objective measures where available (imaging, strength/function tests, standardized scoring)
- Adverse events tracked systematically
- Follow-up duration (did effects persist beyond the immediate window?)
In my work, I’ve found that “improvement” is where evidence often becomes slippery: some studies emphasize short-term changes, while others report longer-term function. Those aren’t interchangeable.
3) Sample size and statistical power
Small studies can be informative, but they’re also where false positives and exaggerated effect sizes are most likely. When you’re reading bpc 157 human trials summaries, check whether the reported conclusions match the study’s power.
Practical test: if the study shows a “dramatic” result but provides limited detail on variance, confidence intervals, or adverse event rates, treat the magnitude with caution.
4) Safety reporting: what was monitored and how?
“I didn’t see problems” isn’t the same as structured safety monitoring. Review whether trials:
- Reported adverse events systematically
- Monitored relevant lab parameters and duration
- Described discontinuations or protocol deviations
This is especially important for peptides and investigational compounds, where dosing, route, and purity can vary widely across sources.
Why human evidence for BPC-157 can look limited—without requiring a cover-up
It’s tempting to interpret a thin human database as deception, but there are several mundane, evidence-compatible reasons investigators may not have produced large, definitive trials.
Translational friction: from preclinical promise to clinical endpoints
Preclinical signals in injury models often don’t map neatly onto human heterogeneity—differences in injury severity, comorbidities, timelines to treatment, and rehab protocols. I’ve watched promising mechanistic work struggle when it meets real-world clinical variability.
Commercial and regulatory incentives can differ by compound category
Human trials require funding, regulatory pathways, and operational feasibility (manufacturing consistency, quality testing, stable dosing regimens). Even when interest exists, the “race” to fund large trials may lag until stronger signals justify the cost.
Importantly, this is consistent with an evidence gap: not nothing is happening, but the scale and quality may not yet be there.
Outcome selection affects whether results ever “look clear”
Trials that measure outcomes poorly—or choose endpoints misaligned with how recovery is experienced—can yield non-significant results even when biological activity is present. In translational reviews, endpoint mismatch is a frequent reason the story fails to resolve.
Critical questions to ask next (a checklist you can use immediately)
Here’s the evidence-focused checklist I use when someone wants to move beyond debate and into evaluation. Use it on any BPC-157 write-up, blog claim, or “trial summary.”
Evidence mapping questions
- How many human studies are there? Name them, and distinguish randomized vs. non-randomized work.
- What are the sample sizes? Are results underpowered or exploratory?
- What exact outcomes were measured? Are they functionally meaningful and assessed consistently?
- Was there a control group? If not, can natural recovery explain the findings?
- What’s the follow-up duration? Is there durability, or only short-term signals?
Quality and transparency questions
- Are methods described clearly? Randomization, blinding, and adverse event definitions.
- Are adverse events reported? Not only “no serious issues,” but actual rates and categories.
- Are protocols registered? If published, do the methods match the published outcomes?
- Are results consistent across studies? Consistency matters more than one impressive anecdote.
Claims-evidence alignment questions
- Does the claim match the endpoint? If a paper measures one outcome, does it overgeneralize to all injury contexts?
- Is the effect size plausible? Especially in small studies, watch for exaggerated interpretations.
- Are the conclusions appropriately cautious? Strong claims should come with strong methods and balanced reporting.
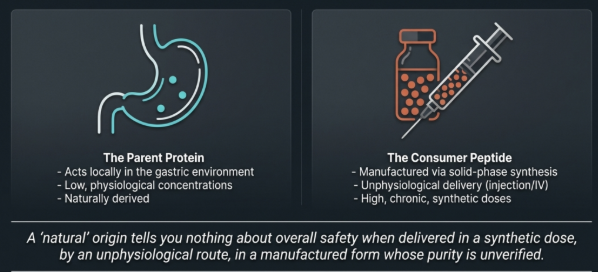
Where imagery and marketing can mislead (and how to stay grounded)
I’ve seen how “story visuals” can reinforce belief before evidence is actually reviewed. An image can’t tell you whether a human trial was randomized, blinded, or adequately powered. It also can’t resolve whether reported outcomes were clinically meaningful.
In my team’s review workflow, we treat visuals as context at most—never as evidence of efficacy or safety. The study design and published outcomes are the evidence.
So, is it an evidence gap or a cover-up?
Based on how evidence typically appears for investigational compounds with limited large-scale clinical programs, the most common explanation is an evidence gap: fewer human trials, variable quality, inconsistent endpoints, and limited replication. That pattern can occur without anyone “hiding” results.
A cover-up claim requires unusually strong, multi-signal proof—especially replication and transparency that would normally surface in legitimate research channels.
The most productive stance isn’t to pick a camp; it’s to demand traceable, high-quality human data and to evaluate studies by design, outcomes, safety reporting, and follow-up.
FAQ
What does “bpc 157 human trials” evidence usually include?
Typically, it includes small human studies (sometimes non-randomized or exploratory) that evaluate specific endpoints related to injury recovery or related outcomes. The key is to examine design quality, control conditions, endpoint validity, adverse event reporting, and follow-up length—not just the existence of a “human” study label.
How can I tell if a BPC-157 claim is based on strong evidence?
Look for randomized or controlled designs, clear inclusion criteria, pre-specified clinically meaningful endpoints, transparent methods, confidence intervals or effect sizes consistent with the sample size, and complete adverse event reporting. Be especially skeptical when claims are broad but the trial outcome measures are narrow or short-term.
What should be my next question after reading about a study?
Ask what follow-up evidence exists: replication, longer follow-up, consistent outcomes across studies, and whether the trial’s endpoint aligns with the real-world clinical goal you care about (function, recovery timeline, and safety).
Conclusion: Move from debate to evidence mapping
The difference between an evidence gap and a cover-up isn’t found in rhetoric—it’s found in the structure and transparency of the human database. For bpc 157 human trials, evaluate studies by design (randomization and controls), endpoints (clinically meaningful recovery measures), safety reporting, sample size, and follow-up duration. When the evidence is limited, that usually explains the uncertainty more directly than conspiracy narratives do.
Next step: pick one recent BPC-157 human trial you’ve seen referenced, and write down—study design, sample size, control type, endpoints, follow-up length, and adverse event reporting. If those aren’t clearly available, that absence is itself an important data point.
Discussion