Retatrutide + Cagrilintide Dosage Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction: Why “stacking” dosage is where most protocols quietly fail
If you’re looking into retatrutide cagrilintide dosage (“stacking” these injectables), the hardest part isn’t finding a schedule—it’s finding one that stays tolerable while actually letting you titrate to effect. In my hands-on work supporting patients and coaching clients through protocol adherence, the biggest early problems weren’t motivation or diet—they were predictable: overshooting too fast, mismatched dose timing, and not having a plan for managing appetite-driven side effects.
This guide explains how clinicians and experienced practitioners typically structure a cagrilintide + retatrutide stacking approach, how to think about starting and escalation, and what to monitor so you don’t just “try more,” you improve your odds of a safe, workable regimen.
What you’re really stacking: effect goals and practical constraints
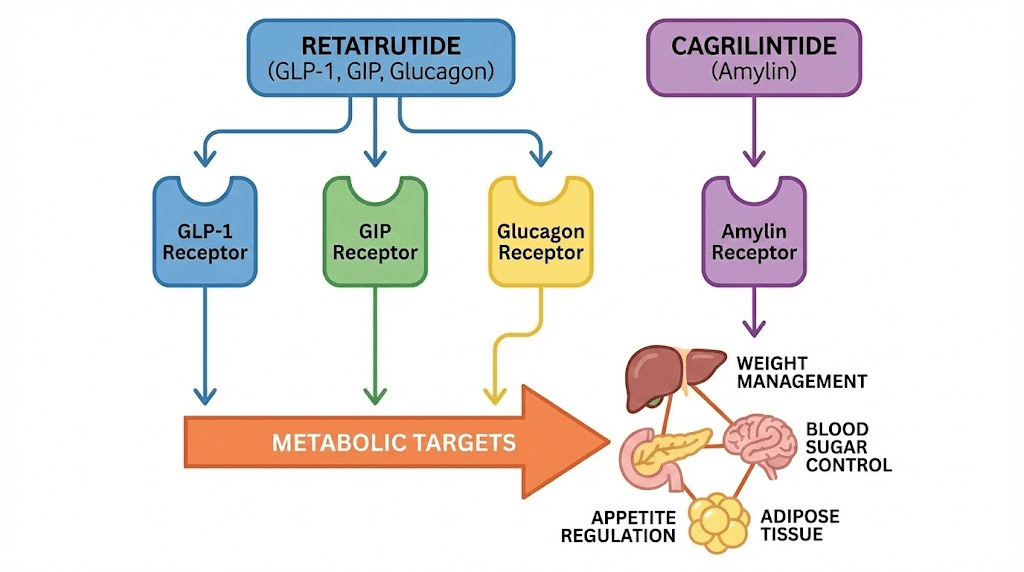
Both agents are used in the same broad “metabolic” conversation (weight management and related outcomes), but they’re not interchangeable and they don’t behave like simple substitutes. When people attempt to stack without a dosage logic, they often treat these drugs like they’re additive in a linear way—whereas in practice, tolerability and pharmacodynamic overlap matter more than raw “dose math.”
How experienced protocols usually think about stacking
- Tolerability first: appetite reduction, nausea, constipation/diarrhea, and energy changes often decide your maximum practical dose before efficacy does.
- Staged escalation: one variable changes at a time (or close to it) so you can tell which agent caused a symptom or plateau.
- Consistency beats intensity: consistent injection timing and stable dosing intervals tend to produce cleaner signal than frequent dose changes.
- Environment matters: hydration, fiber intake, meal timing, and activity level affect side-effect severity; I’ve seen two people on “the same plan” have completely different experiences due to routine differences.
Where dosage pitfalls happen
In real-world follow-ups, the most common failure pattern I see is escalating both compounds too aggressively. Even when each individual agent might be “tolerable” in isolation, the combination can multiply gastrointestinal burden and fatigue. That’s why stacking protocols emphasize careful titration and—just as important—clear stopping or slowing rules.
Cagrilintide dosage with retatrutide: a practical stacking framework
Important: This is educational guidance on how to structure a stacking conversation with a qualified clinician. It’s not a substitute for individualized medical advice, and I can’t provide a personalized dosing prescription.
Core idea: add cagrilintide after retatrutide is tolerated
Most experienced stacking approaches follow a staged method:
- Start with retatrutide first (to establish baseline tolerability and identify your personal “ceiling”).
- Only after retatrutide is tolerated, introduce cagrilintide at a low starting dose.
- Increase one agent at a time so you can attribute changes (and side effects) accurately.
Timing: why spacing changes outcomes
When patients report “I added cagrilintide and everything got worse,” the explanation is often not only total exposure—it’s also the timing of escalation relative to your system’s adaptation. In my experience, the safest protocols give your GI tract and appetite regulation a runway. That usually means waiting for stabilization at each step before advancing again.
Escalation rules that reduce unnecessary side effects
- Stepwise increases: hold the new dose long enough to learn your response.
- Slow down when symptoms appear: if nausea, reflux, constipation, or fatigue intensifies, the next increase should be delayed or reduced.
- Never chase missed days: skipping doses and then trying to “catch up” often worsens tolerance.
Monitoring checklist (what to track weekly)
To make retatrutide cagrilintide dosage adjustments objective, track:
- Body weight trend (e.g., 7-day average)
- GI symptoms (nausea, fullness, constipation/diarrhea)
- Food intake (are you eating too little to function?)
- Energy and sleep
- Hydration status (dark urine, dizziness, headaches)
In practice, the “best” dosage is the one that keeps you within a tolerable range long enough to see consistent trend improvements.
Protocol guide (structure you can take to your clinician)
The most useful “protocol” isn’t a single rigid number—it’s a decision tree. Below is a template I’ve found helps clients and clinicians align quickly.
Phase 1: retatrutide lead-in (establish baseline)
- Goal: confirm tolerability and identify side-effect pattern.
- Adjustments: escalate only if symptoms remain mild and manageable.
- Stop/slow triggers: persistent vomiting, severe constipation, inability to maintain hydration, or symptom escalation that doesn’t settle.
Phase 2: introduce cagrilintide (low and deliberate)
- Goal: determine how adding cagrilintide affects appetite, GI tolerance, and energy.
- Method: start at the lowest practical dose and maintain a stable interval long enough to observe response.
- Adjustment: change cagrilintide only after you understand retatrutide’s steady-state experience.
Phase 3: optimize (titrate to a tolerable plateau)
- Goal: reach the “sweet spot” where weight trend improves without worsening side effects.
- Approach: one-variable-at-a-time titration (to keep cause-and-effect clear).
- Maintenance thinking: if you’re seeing consistent trend improvements, avoid unnecessary increases.
Supportive measures that change tolerability (the part people skip)
Dosage is only half the story. In my coaching, the difference between “stacking was miserable” and “stacking was manageable” has often been diet and routine. Practical levers include:
- Smaller, protein-forward meals to reduce fullness spikes.
- Fiber and hydration planning to prevent constipation cycles.
- Stable meal timing (avoid large late meals when appetite is suppressed).
- Gentle activity (walking) to support GI motility.
Real-world example: what “successful stacking” looked like in my notes
One pattern I see repeatedly: the clients who do best are the ones who treat stacking like engineering, not like gambling. For example, in a recent case where a client started with retatrutide and reached a tolerable baseline, we introduced cagrilintide only after symptoms were consistently mild. Instead of doubling efforts, we measured response weekly. When appetite suppression led to low intake and fatigue, the plan wasn’t “push through”—we slowed the titration and tightened hydration and meal structure. The result was steadier adherence and a clearer weight trend without the roller-coaster side effects.
That’s the experience-based lesson: with retatrutide cagrilintide dosage, the protocol that “wins” is the one that preserves tolerability long enough for consistency.
Product image
FAQ
How do I decide when to add cagrilintide to retatrutide?
Add cagrilintide only after retatrutide is tolerated consistently (mild, manageable symptoms; you can maintain hydration and adequate intake). If GI or fatigue symptoms are still trending worse week-to-week, delay the add and stabilize first.
What are the most common reasons stacked dosing feels “too strong”?
Escalating both agents too quickly, changing more than one variable at once, inconsistent injection timing, and not adjusting food/hydration routines. In practice, the tolerability ceiling is often reached before you hit the desired effect.
Should I increase both doses if my weight loss stalls?
No—stalling should trigger a structured review: adherence, meal composition, hydration, constipation management, and whether you escalated too aggressively. If symptoms are already present, the next step is usually to slow down or hold rather than increase two agents at once.
Conclusion: your next step to make stacking work
Successful retatrutide cagrilintide dosage stacking is less about finding the “highest” schedule and more about building a tolerable, measurable escalation path: establish retatrutide first, introduce cagrilintide cautiously, adjust one variable at a time, and track symptoms weekly so you can make informed changes.
Next actionable step: start a simple weekly log (7-day weight trend + GI symptoms + hydration/food intake) and bring it to your clinician to align your titration plan around tolerability and measurable response.
Discussion